Download

1 / 28
310 likes | 481 Vues
Continence issues in school. June Rogers MBE Paediatric Continence Advisor Director PromoCon, Disabled Living, Manchester www.promocon.co.uk 0161 834 2001. What are the issues??. What problems may be encountered in school?. ‘Normal’ delayed acquisition of bladder control

E N D
Continence issues in school June Rogers MBE Paediatric Continence Advisor Director PromoCon, Disabled Living, Manchester www.promocon.co.uk 0161 834 2001
What problems may be encountered in school? • ‘Normal’ delayed acquisition of bladder control - Not uncommon in nursery age children. - School staff need to be reassured - Structured day helps facilitate training - delayed training associated with LD may need more structured training
What problems may be encountered? • Day-time wetting (diurnal incontinence) - not uncommon affecting 5% of 5 year olds - need to be aware outside child’s control - will require formal intervention involving regular fluid intake and toileting - free access to both should be facilitated
What problems may be encountered ? • Bedwetting (Nocturnal Enuresis) - obviously does not occur during school day but impact of wetting and any treatments will - child will need regular drinks and access to toilet - morning bath/shower may make child late - use of enuresis alarm may make child tired next day
What problems may be encountered? • Soiling - most commonly related to constipation - soiling therefore outside child’s control - child make be at risk of bullying and name calling - school to ensure privacy and easy access to toilet
What problems may be encountered? • Continence problems related to an acquired or congenital disability - an increasing number of such children now in mainstream school population - multi-disciplinary approach often required - named carers need to be identified - individualised training programmes
Children with continence problems • Good practice in continence services (DH 2000) – Joint targets for health and local authorities: children • Managing Medicines in Schools and Early Years Settings (DH March 2005) • ‘Including me’ Managing complex health needs in schools and early years settings (Oct 2005)
Good practice in continence services, DH 2000 Schools need to: • Preserve dignity and independence and avoid risk of ridicule and bullying • Carry out continence treatment /management plan as agreed in assessment • Enable good pathways of communication • Provide adequately trained school-based care staff
A good school continence policy should: • Place continence in the context of disability discrimination legislation • Give a commitment to include this group of children in all activities • Maintain the dignity, independence, need for privacy and self esteem of child • Be linked to an anti-bullying policy • Define health and safety issues
A good school continence policy should: • Outline the facilities which need to be in place • Adapt facilities to encourage independence and ensure privacy • Define procedures and protocols….which should be child centred • Highlight the child protection issues which need to be taken into account
‘Less favourable treatment’ ‘Blanket’ school policies can be seen as discriminatory and therefore unlawfull • A mother seeks admission to a nursery school for her son who has Hirschprung’s disease. The school says that they could not admit him until he is toilet trained. That is their policy for all children… The refusal to admit the boy is for a reason related to his disability and is potentially discriminatory
Questionnaire sent to schools • To identify teachers’ past experiences and knowledge of wetting and soiling problems in children • To explore teachers’ views and acceptance of inclusion of children with wetting and soiling problems in school • To identify the involvement of any health professional e.g. school nurse
Results - teacher perspective • All but 2 of the schools had had previous experience of children with incontinence • No specific training undertaken of toileting issues within post-grad education • Unclear expectations regarding age of attainment of toilet training • Lack of awareness regarding causes of wetting/soiling problems
Results - health perspective • Only 40% of teachers had been given any information regarding the child’s problem • 50% felt information not sufficient • 77% of children did not have a written care plan • 95% of staff had not had specific training to help manage the child’s problem • poor facilities for changing/toileting
Steps in child specific training It is always necessary for child specific training to include: • An overview of the child’s condition so staff aware of rationale of the procedure • The specific health care procedures • A plan to cover unexpected happens and what to do in an emergency
Overview of training • Description of condition and required procedure • Psychosocial implications –privacy confidentiality and dignity. Involvement of child in care and preferences • Information from IHCP • Communication network
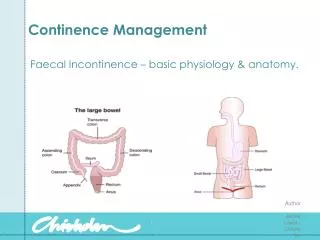
Health Care Procedures • Basic Anatomy • Purpose of procedure • Emergency plan • Timing • Teaching method • Procedure location • Universal precautions • Equipment and supplies required • Lifting and position • Child’s involvement in self care • Precautions • Signs and symptoms requiring attention • Documentation of procedure • Scheduled supervision and follow up
Promoting independence • Increase tolerance for care – appropriate goals to be developed • Involving the child – the use of ‘smart cards’ may be helpful • Achieving independence – degree of support / supervision will vary according to needs of the child
Implementation, monitoring and evaluation • Provision / supervision of care – majority of cases care delegated to school staff…needs to be clear who to contact in case of emergency • Annual update of child’s needs – health care procedures to be reviewed annually • Documentation and update skill training – provides a clear understanding of required health care needs
Clean Intermittent catheterisation • Organisation of programme – identifying individual children’s needs • Care staff – selecting staff and appropriate training / supervision • Responsibilities – school and parents • Developing an Individualised Health Care Plan (IHMP)
Individualised Health care Plan – need to consider such as : • Flexible timing of catheterisation • Individual baseline status • Position of child • Type of catheter and instructions for use • Child’s ability to participate in procedure • Potential problems that may arise • Latex allergy alert • Infection control • Moving & handling implications
Review emergency plan to include: • Signs of possible problems • Response to problems and emergency situations • Individual responsibilities • Location of emergency plan • List of people to contact in an emergency
Transition • “16 is an age when there is lots of other change. When moving schools, it happens at the same time to everyone and changing schools is hard enough - but changing consultants and hospitals is even harder because you are doing it on your own and doing it because you are suffering from a serious illness” (young person attending conference).
Good transitions - what young people say they want. • Consider the timing; plan early and prepare for leaving and arriving at different service. • Take into account how attitudes, thinking and behaviour vary between individual young people. • Involve young people in service design and delivery: provide opportunities for young people to ask questions, express opinions and make decisions. • Provide accessible information about services; share information between services; ensure multi agency working
Good transitions - what young people say they want… • Stress the importance of a trusted adult who can challenge and support them, act as advocate and help them to develop self-advocacy skills. • Establish a shared philosophy between adult and paediatric care including schools. • Adopt an individualised honest approach. • Address loss of continuity of care at transition; ensure new relationships are established. • Train professionals in adolescent health in both paediatric and adult sectors.