Download
1 / 92
920 likes | 938 Vues
Learn about the anatomy and important structures of the neck triangles including detailed descriptions of the anterior and posterior triangles. Explore key landmarks and features in this comprehensive guide.

E N D
Triangles of the neck The neck is divided by the sternocleidomastoid muscles into: anterior and posterior triangles.
Anterior triangle of the neck • The anterior triangle is bounded laterally by the SCM muscle, medially by the midline, and superiorly by the mandible. • The anterior triangle can be further divided into carotid and submandibular triangles. • In the carotid triangle the carotid pulse may be felt. • In the anterior triangle the hyoid bone can be palpated. • On swallowing the hyoid bone can be felt to rise. • As the hyoid rises it pulls with it the thyroid cartilage which forms the Adam's apple.
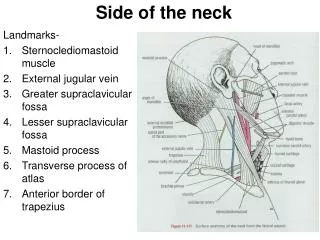
Posterior triangle of the neck • The posterior triangle is bounded posteriorly by the trapezius muscle, anteriorly by the SCM. muscle and inferiorly by the clavicle. • Much of the cervical nerve plexus emerges in the posterior triangle. • The spinal accessory nerve runs subcutaneously across the posterior triangle from the posterior border of SCM to the anterior border of trapezius. It supplies both muscles
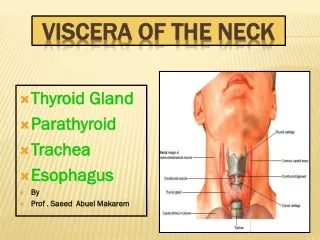
Triangles of the neck • Anterior triangle of the neck • thyroid isthmus • Posterior triangle of the neck • Spinal accessory nerve • Brachial plexus • Subclavian artery-third part • External jugular vein • Parotid gland
Triangles of the neck • A. Anterior triangle • muscular triangle--formed by the midline, superior belly of the omohyoid, and SCM • carotid triangle--formed by the superior belly of the omohyoid, SCM, and posterior belly of the digastric • submental triangle--formed by the anterior belly of the digastric, hyoid, and midline • submandibular triangle--formed by the mandible, posterior belly of the digastric, and anterior belly of the digastric • B. Posterior triangle • supraclavicular triangle--formed by the inferior belly of the omohyoid, clavicle, and SCM • occipital triangle--formed by inferior belly of the omohyoid, trapezius, and SCM
Anterior triangle of the neck • Above the thyroid cartilage, is the hyoid bone. • Below the thyroid cartilage in the midline is the cricoid cartilage. • The trachea continues on from the cricoid cartilage. • The cartilages of the trachea can be felt until it enters the thorax behind the manubrium. • The trachea can be moved from side to side. • The thyroid gland lies on either side of the trachea and crosses it anteriorly at about the second ring. • The thyroid is covered anteriorly by the thin strap muscles and lies in part under the SCM. muscles.
Anterior aspect of the neck • Body of the hyoid bone • Thyrohyoid membrane • Upper border of the thyroid cartilage • Cricothyroid ligament • Cricoid cartilage • Cricotraheal ligament • First ring of the trachea • Isthmus of the thyroid gland • Suprasternal notch
Posterior aspect of the neck • External occipital protuberance • Nuchal groove • C7 spinal process
Carotid sheath • Carotid artery • Internal jugular vein • Vagus nerve • Deep cervical lymph nodes Marked out by a line joining the sterno-clavicular joint to a point midway between the tip of the mastoid process and the angle of the mandible. At the upper border of the thyroid cartilage, CCA bifurcates into the internal and external branches. The pulsations can be felt at this level.
Carotid sheath- common carotid artery, internal jugular vein, vagus nerve with its superior laryngeal branch
Common carotid artery: external carotid artery, internal carotid artery Branches of ECA: superior thyroid artery , superior laryngeal artery, lingual artery, facial artery.
Lumps in the neck 1. Lymph nodes- lymphadenopathies: • Infections • Metastatic tumors • Primary tumors 2. Tumors- cystic or solid 3. Thyroid gland- Goitre- diffuse or nodular
Case report • Patient: An 8-year-old girl, Address: country side of Chiang Mai province • CC : Fever for 10 days and sore throat for 6 days • History > 10 days , she had an acute onset of high-graded fever. She took paracetamol but the fever and headache remained. > 6 days, she was seen by a doctor who gave a diagnosis of acute tonsillitis (injected and enlarged tonsils, body temperature 40 C, • CBC: Hb 11.0 gm%, HCt 34%, WBC 4,600/cu.mm, N 68%, B 1%, L 29%, platelets 177,000/cu.mm).
Case report • She was given intramuscular lincomycin 450 mg and oral amoxycillin 250 mg 3 times a day. High intermittent fever persisted. • > 2 days, she developed rashes over the trunk, arms, and thighs. She also had various nonspecific symptoms, including faintings, mild nausea, periumbilical abdominal pain, diarrhea, mild sore throat, nonproductive cough, and severe bitemporal headache. • > On admission day, the fever persisted and her sore throat got worse
Case report • Past History: The girl had history of cleft lip and cleft palate which were repaired since she was 3 months old. • Her immunization status was up to date. • There was no family history of similar illness. • She usually plays around her house where grass and tree wildly grow on humid ground.
Physical examination VS: T 39.5 C, pulse rate108/min, RR 24/minm, BP=100/60 mmHg., BW 20 Kg GA: looked sick, but fully concious Skin: faint maculopapular rashes were observed over arms and thighs . An ulcer with black crust on erythematous base was seen over her right shoulder region . Its size was approximately 8.0 mm in diameter. The lesion was not tender.
Lymphadenopathy • Multiple enlarged lymph nodes were palpated as follows: • 2 large: 1,3 and 1,2 cm. in diameter on right supraclavicular triangle • Multiple small lymph.nodes<5mm.in diameter in chain along both sides of posterior triangle All nodes were soft, not-tender, movable and smooth surface
Case report • ENT examination revealed enlarged tonsils grade III/IV with hyperemia which extended on anterior tonsillar pillars and soft palate were detected. There was no exudative patch. Her pharynx was not injected. Her conjunctiva was normal.Chest: Heart sound: WNL, Lungs: no adventitious soundAbdomen: palpable liver (4 cm below right costal margin, span 13 cm.), spleen was not palpable NS: WNL
Case report • Active Problem list: 1. Prolonged fever for 10 days 2. Nonspecific systemic complaints: faintings, nausea, abdominal pain, diarrhea, sore throat, cough, headache, poor appetite 3. Generalized maculopapular rash 4. Cervical and supraclavicular lymphadenopathy 5. Injected and enlarged tonsils with hyperemic soft palate 6. A black crusted ulcer at the right shoulder 7. Hepatomegaly
Case report • Initial laboratory investigations: CBC: Hb 9.2 g/dl, Hct 28 %, WBC=5,200/cu.mm (N 80%, L 20%), platelets 131,000/cu.mmPeripheral blood smear for malarial pigment: negativeU/A: WNL
Case report • Since the provisional diagnosis of "scrub typhus" was made, the therapeutic diagnosis was started with oral doxycycline 2.2 mg/kg/dose given every 12 hrs (for the first 2 doses) . • The fever dramatically subsided. • Twelve hours later, she became more cheerful and her appetite returned. Therefore, doxycycline (2.2 mg/kg/day div q 12 hrs) was continued. • The hyperemic soft palate and tonsils subsequently faded off. The tonsils were slightly decreased in size 36 hours after doxycycline. • The lymph nodes and liver remained palpable at the time of the discharge from the hospital on day 3 of the treatment. Doxycycline was continued for 14 days.
Case report • Follow-up: Seven days after the discharge (10 days after doxycycline) she was followed up. • She was afebrile and had no rash. The lesion (eschar) moderately reduced in size. • Her tonsils and lymph nodes became normal size for age. Liver was just palpable below right costal margin.
Discussion • Scrub typhus is a febrile illness caused by Orientia tsutsugamushi, an obligate intracellular bacterium in the Rickettsiaceae family. • The organism is transmitted during the bite of trombiculid mites (chigger). Field rodents are the reservoir hosts. Scrub typhus is confined to a definite geographic region. It extends from northern Japan and far eastern Russia in the north, to northern Australia in the south, and to Pakistan and Afghanistan in the west. • In 2000, there were 3,914 cases (6.34 cases per 100,000 population) of scrub typhus reported to the Thai Ministry of Public Health (MOPH). • The true incidence is probably much higher since tests for anti-O. tsutsugamushi antibody are available in only a few medical centers in Thailand
Case report • Diagnosis and differential diagnosis of a patient with "eschar " Although this case had no serologic verification, the course of illness, systemic manifestations, a typical eschar, and therapeutic response led to the diagnosis of scrub typhus without difficulty. • Tularemia, spotted fever rickettsiosis, and anthrax can present with eschars but by the epidemiology and clinical course they could be excluded in this case. • Eschar is a very useful sign in making the diagnosis. • Eschar, if carefully searched, was seen in 25-75% of patients with scrub typhus
Case report • Where should we search for? "eschar" • Eschar occurs as the result of mite (chigger) bite. Since the chigger is small (<5 mm) and the bite is neither painful nor itchy, the history of the bite was not usually obtained. • The mite lives in bushes.
Case report • How can scrub typhus present with tonsillitis? • After mite bite (inoculation) the rickettsiae multiply and spread to the adjacent lymphoid structures. • The lymph nodes from the neck/shoulder region drained into nearly ipsilateral superficial cervical lymph node and deep cervical lymph node. Then, there are communications from intraoral structure (tonsil and nasopharynx), cervical lymph nodes, to the the contralateral neck. • Tonsillitis, cervical and supraclavicular lymphadenopathy in this case, represented the regional lymphadenopathy in scrub typhus
Case report • Patient: A 9-year-old HIV-infected girl Address:Payoa province (Northern Thailand) • CC: Pain at both eyes for 4 weeks. Fever for 3 weeks. • Present Illness: 4 weeks PTA, after coming back from swimming in a river, she started having pain at her both eyes (more on the left side). The pain later accompanied with tearing, yellowish discharge and photophobia. The eye drop medicine from the local hospital could not relief her eye pain. • 3 weeks PTA, she developed moderate grade fever and mild dry cough. • Her eye pain persisted. • She lost her appetite and was admitted to a hospital where she received ceftriaxone 70MKD, and ampicillin for 1 week without improvement.
Case report • 1 week PTA, all symptoms persisted and she started having abdominal pain. • Past medical history: • At the age of 3 years she was diagnosed as having HIV infection. • Her mother has a history of pulmonary tuberculosis and has been on treatment for 7-8 months. • She has not gained weight for 1 year.
Case report • Physical examination: • GA: febrile, thin and fatigue. BW=18 kg • Vital signs: T: 40 celcius, RR: 36/min, PR: 122/min, BP: 110/72 mmHg • EYES; pale and injected conjuctivae, left corneal ulcer and photophobia. • Oral cavity; whitish patches (thrush) • Ears; intact both tympanic membranes • Lymph nodes: Right supraclavicularlymphnodeenlagement: 2 cm in diameter, firm, not tender
Case report • Heart: Tachycardia, no murmur • Lungs: Medium creppitation both lungs • Abdomen: Distension, generalized mild tender, liver 4 cm below RCM, • Extremities: no clubbing of fingers • Skin: hypo- and hyperpigmentation scars at extremities. • Neurological examination: no meningial sign, no neurological deficit