Download
1 / 17
170 likes | 265 Vues
FDA 2004: Revisiting the 1996 Obesity Drug Guidance. David G. Orloff, M.D. Division of Metabolic and Endocrine Drug Products, CDER. 1996 Obesity Drug Guidance. Patient Population Body Mass Index (BMI) 27 – 29.9 kg/m 2 with comorbidities (i.e., HTN, DM2)

E N D
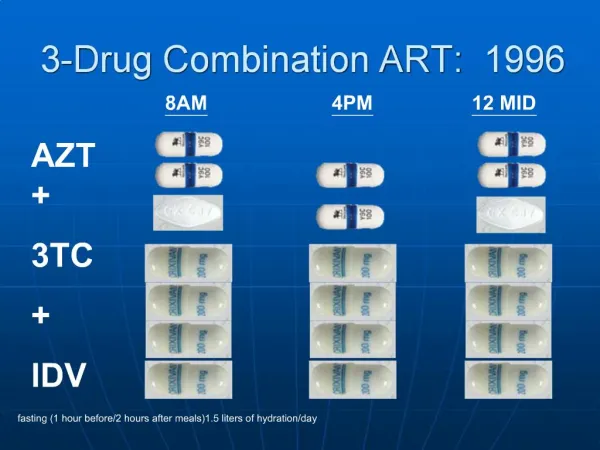
FDA 2004: Revisiting the 1996 Obesity Drug Guidance David G. Orloff, M.D. Division of Metabolic and Endocrine Drug Products, CDER
1996 Obesity Drug Guidance • Patient Population • Body Mass Index (BMI) • 27 – 29.9 kg/m2 with comorbidities (i.e., HTN, DM2) • > 30 kg/m2 without comorbidities • Run-in phase • Identification of placebo-responders • Avoidance of treating unnecessarily with drugs • Duration of Phase 3 Studies • Historical “bad luck” with anti-obesity drugs • Absence of outcomes data • First year placebo-controlled: proof of principle of efficacy • Second year open-label: durable efficacy and safety in long-term use
1996 Obesity Drug Guidance • Efficacy criteria at end of year 1: presumed reduction in risk for sequelae with modest (sustained) weight loss in serious obesity • Mean placebo-subtracted weight loss > 5% • Proportion of subjects who lose > 5% of baseline body weight is greater in drug- vs. placebo-treated group • EMEA criteria at end of year 1: • Mean placebo-subtracted weight loss > 10% • Proportion of patients who lose > 10% of baseline body weight is greater in drug- vs. placebo-treated group
1996 Obesity Drug Guidance • Patient Exposure • 1500 patients completing one year of placebo-controlled exposure • 200-500 patients completing a second year of open-label exposure • ICH E1A • Drugs for long-term treatment of non-life-threatening conditions: • 300 – 600 for 6 months • 100 for one year
ICH E1A : Exposure requirements dictated by demonstrated efficacy • Larger/longer exposures if benefit of drug is: • Small (e.g., symptomatic improvement, less serious disease) • Experienced by only a fraction of treated patients (prevention) • Of uncertain magnitude (reliance on a surrogate) • Average placebo-subtracted weight loss of drugs evaluated to date 3-5% of baseline at year 1 • Not all treated patients lose weight; some gain • Scant data to date from controlled trials of benefits in terms of irreversible morbidity • XENDOS (Orlistat) • No data on cardiovascular morbidity or mortality • SCOUT (Sibutramine)
2004: revisiting the guidance • Charge from Dr. McClellan to OWG/Therapeutics (8-03) • “…[assess] real or perceived barriers to development of new or enhanced therapeutics” • “Make recommendations… on…ways to encourage development of new or enhanced therapeutics” • Growing public health problem • Advancing science • Multiple new drugs in development; anticipated explosion in development programs in coming years • Multiple novel mechanistic approaches • FDA’s role in assuring that safe and effective drugs are efficiently and effectively brought forward through development to marketing for use in the treatment of human disease
2004: revisiting the guidance • Goals • Guidance appropriate for development of drugs, with respect to: • Potential roles of drugs in treatment and prevention • Target populations at risk for obesity and its sequelae • Evidentiary standards for proof of meaningful efficacy • Evidentiary standards for demonstration of acceptable safety
2004: revisiting the guidance • Federal Register Notice • January 26, 2004 • Request for public comment on the 1996 Obesity Drug Guidance • Response • Approximately 17 submissions to the docket • Nearly all from industry
Issues raised in comments • Broadening of target population • Adolescents • Burgeoning problem • Long-term, population-specific risks (i.e., linear growth, bone) • Most appropriate endpoint (i.e., BMI rather than weight) • (Specific criteria for selection not proposed) • Lower BMI limit targeting prevention of weight gain • “High-risk” treatment and prevention (without specifics) • Drugs “effective” in those with lesser degrees of obesity • Diabetes, Metabolic syndrome (these are not excluded based on trials to date)
Issues-2 • Study design • Run-in • Proof of efficacy only in those unable to lose weight on diet/exercise is an excessive standard • More generalizable results if no run in required • Measure of effect is placebo-subtracted weight change from baseline • (means of assuring standard of care in context of trial not addressed)
Issues-2 (con’t) • Duration • One year of controlled efficacy • Safety at one year • Questionable utility of additional year if no safety concerns after 1st year • (Approach to assessing need for additional time or patients not addressed) • Controls/Combination studies • (Efficacy criteria not addressed)
Issues-3 • Efficacy criteria • Total weight loss > 5% from baseline at 12 months • Placebo-subtracted weight loss > 5% from baseline at 12 months (current criterion) • Significantly greater proportion (drug vs. plbo) losing > 5% of weight at 12 months (current criterion) • Define categorical win more specifically (i.e., absolute or relative difference in percentage of patients achieving 5% or greater weight loss)
Issues-3 (con’t) • Efficacy criteria • Define weight maintenance • Define prevention of weight regain • Define drug-induced weight gain • BMI in pediatric patients
Issues-4 • Safety exposures • Arbitrary • Current obesity guidance • 1500 patients for one year; 200-500 for second year • ICH • 100 patients for one year
Summary/Points for discussion • Populations • Lower entry criterion to a BMI > 25 kg/m2 when accompanied by comorbidities* • What evidence supports treatment or prevention in this population? • What magnitude of effect would be clinically significant? • What assurance of safety is required to treat lower-risk patients? • Pediatric/adolescents • What factors should be weighed/addresssed in assessing risk vs. benefit? • Obesity-associated metabolic derangements/cv risk factors as primary targets of drug therapy
Summary/Discussion-2 • Design • Run-in prior • Identification of pbo responders • Avoidance of unnecessary tx • Standard of care • Combination drug regimens • Standards of efficacy • Endpoints • Define obesity prevention, weight maintenance, prevention of weight regain* • Are these distinct clinical effects? • Are these distinct pharmacological effects? • Are studies needed to document efficacy and safety in each? • Include requirements for approval of treatment or prevention of drug-induced obesity* • Data on risks for and associated with drug-induced obesity, by drug • Issues of interactions impacting safety and efficacy • Criteria for efficacy • Include a section on treatment of obesity in pediatric patients*
Summary/Discussion-3 • Reduce the number of patients in phase 3 study from 1500 examined over one year to 500 – 1000, or even fewer* • Rationale based on magnitude/nature of efficacy? • Rationale based on size of target population? • Rationale based on expectations regarding safety? • Eliminate the second year of open-label study* • Rationale based on nature of drug “toxicities”: acute vs. cumulative? • Suggested changes • Require an absolute difference for the categorical weight loss criterion • Include metabolic syndrome as a therapeutic endpoint • Include requirements for approval of drug combinations • Cosmetic weight loss • Psychological benefits • Social/economic benefits • QOL