Download
1 / 50
500 likes | 785 Vues
Anterior Ankle Impingement in Gymnasts. Jon Fravel, MS, ATC/L. Overview. Clinical Interest Anatomical Descriptions Etiology Gymnastics Overview Conservative Treatment Surgical Summary. Clinical Interest. Ankle injuries are very common in sport

E N D
Anterior Ankle Impingement in Gymnasts Jon Fravel, MS, ATC/L
Overview • Clinical Interest • Anatomical Descriptions • Etiology • Gymnastics Overview • Conservative Treatment • Surgical Summary
Clinical Interest • Ankle injuries are very common in sport • As an outsider a few years ago it seemed there were quite a few gymnasts with ankle “issues” • First case I was involved with at the Univ of Iowa
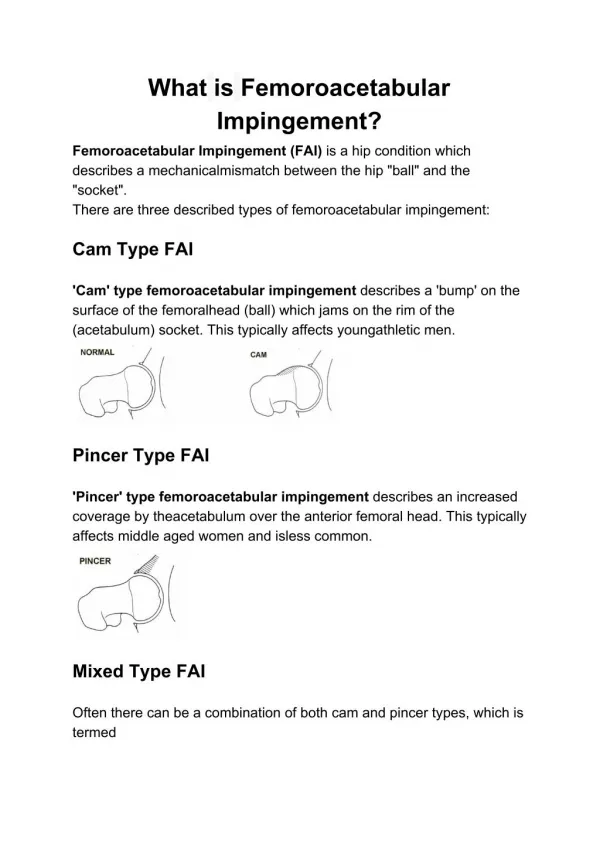
Defining Anterior Ankle Impingement • Footballers Ankle • Morris & McMurray • Chronic anterior ankle pain is commonly caused by talotibialosteophytes at the anterior portion of the ankle joint. • In general, osteophytes are the secondary manifestation of osteoarthriticchanges. However, repetitive minor trauma in the ankle, as seen in athletes, can induce spur formation, with radiographic characteristics similar to osteophytes. – van Dijk
Etiology • Footballers Ankle (Traction Spurs) • The anterior joint capsule attaches on the tibia at an average of 6 mm proximal to the joint level • On the talar side, the capsule attaches approximately 3 mm from the distal cartilage border • The distance of capsular attachment to the most frequent location of bony spurs is thus relatively large • Traction spurs from recurrent traction to the joint capsule is not plausible • On top of this during arthroscopy the spurs are found within the capsule • van Dijk 2006. Tol JL, van Dijk CN. Etiology of the anterior ankle impingement syndrome: a descriptive anatomical study. Foot Ankle Int 2004;25:382–6. • van Dijk CN, Tol JL, VerheyenCC.Aprospective study of prognostic factors concerning the outcome of arthroscopic surgery for anterior ankle impingement.Am J Sports Med 1997;25: 737–45. • Tol JL, Verheyen CP, van Dijk CN. Arthroscopic treatment of anterior impingement in the ankle. J Bone Joint Surg Br 2001;83:9–13.
Footballer’s Ankle • Examination of video showing only a minority of individuals actually reached full plantarflexion during kicking. • Likely bones response to the trauma of the ball contacting the tibia and the talus. • Tol 2002
Etiology • O’Donohue (1957) considered the osteophytes to be related to direct mechanical trauma associated with the impingement of the anterior articular border of the tibia and the talar neck during forced dorsiflexion of the ankle. • Bone formation is considered to be a response of the skeletal system to intermittent stress and injury • Wolff’s law of bone remodeling • O’Donoghue DH. Impingement exostoses of the talus and tibia. J Bone Joint SurgAm1957; 39-A:835–52.
Etiology • In cadavers a triangle of soft tissue- synovial fold, synovial fat, and collage tissue were found along the anterior jt line. • Repetitive trauma may cause hypertrophy of the synovial layer and and create subsynovial fibrotic tissue also causing infiltration of inflammatory cells. • These osteophytes decrease anterior space and compression of this tissue is more likely to occur. • BerberianWS, Hecht PJ, Wapner KL, et al. Morphology of tibiotalarosteophytes in anterior ankle impingement. Foot Ankle Int 2001;22:313–7. • FerkelRD, Karzel RP, Del Pizzo W, et al. Arthroscopic treatment of anterolateral impingement of the ankle. Am J Sports Med 1991;19:440–6.
Posterior Ankle Impingement • Chronic posterior ankle pain is commonly caused by an ostrigonum or other bony impediment • hypertrophic posterior process of the talus. • Hyperplantar flexion (with dancers en pointe or demipointe but with research does not seem to be the case) • Traumatic event plus this hyperdorsiflexion to cause post ankle impingement • (hard floors, ankle sprains, supinationtrauma) • Posterior talarprominence becomes compressed between the tibia and the calcaneus during forced plantarflexion. In the presence of an ostrigonum, this can lead to micromotion of the ostrigonum, and pain.
Who • Typically, patients with an anterior ankle impingement are relatively young athletes with recurrent inversion injuries of the ankle • St Pierre RK, Velazco A, Fleming LL. Impingement exostoses of the talus and fibula secondary to an inversion sprain. A case report. Foot Ankle 1983;3:282–5. • Pt present with anterior ankle pain, swelling after activity, and (slightly) limited dorsiflexion. The diagnosis of anterior impingement is clinical, based on physical examination. Recognizable local pain on palpation is present anteriorly, and the osteophytes may be palpable with the ankle joint in slightplantarflexion. • Van Dijk 2001 • If pain is anterormedial with palpation it is consieredanteromedial impingement. If pain is anterolateral with palpation it is considered anterolateral impingement • Forced dorsiflexion can often provoke pain but sometimes false negatives.
Gymnastics • Quite a few injuries in gymnastics • Each gymnast reported an average of 3.64 injuries per 12 month period • 4.19 for the elite gymnasts and 3.30 for the subelitegymnasts • In relation to training hours: the elite gymnasts reported 2.63 injuries per 1000 training hours while their subelite counterparts reported 4.11 injuries per 1000 hours • Kolt and Kirby 1999
Univ of Iowa Gymnastics • Over the past 1 yr we’ve had 3 surgical cases on the men’s and women’s gymnastics teams. • Most bilateral but not all. • 2 more likely scheduled for the end of this year. • 1/5 male
Univ of Iowa • As I work mostly with the women’s team I reviewed the hx of all of the women’s team over the past 3 yrs. • For that population 10/26 have been diagnosed with these anterior impingement. • 38.5%
How does this compare? • How do you define injury? • 1 NCAA • Result from participation in practice • AND Require attn from ATC or MD • AND Restricted participation for 1 or more days • 2 Kolt and Kirby (18 mos prospective survey) • Also reviewed injury studies • Snook- Bring attn to a doctor • Sands- Damaged body part that affected training
How does this compare? • Actual answer is we don’t know. • When asked gymnasts say it is not uncommon. • Kolt and Kirby say 30.7% of the injuries are foot and ankle. • NCAA ISS 88-89 thru 03-04 • 23.0% foot and ankle at competition • 18.2% foot and ankle at practice
When do we see these injuries? • Unscientific and not a lot of evidence to base this on • Women/girls earlier than men/boys • Why? Two thoughts. • Age at peak • Training • Intertwined....
Age at Peak • Females in the US peak elite at 15.7 yrs • Must be 16 for Olympics by December of that year. • (US levels) USA Gymnastics • 1-3 (not often done) • 4-10 (belt system in karate) accomplish certain skills or certain scores • Elite • International elite FIG (Federation InternationaleGymnastique) • Most College gymnasts are Level 10, Elite, or International Elite. • Very few international elites at Univ of Iowa.
Training and Misc • Problem with men as well, but is more frequently seen with women (in my experience) • Men have 6 events • FX, PH, SR, V, PB, HB (Olympic Order) • Women have 4 events • V, UB, BB, FX (Olympic Order) • Both w/ 2 most LE events • Men spend a different ratio of time dedicated to UE events • Ring strength, pommel strength. • Years to be able to swing pommels.
Training and Misc • Unfortunately no longer have an NCAA ISS for MGM • @ Iowa 294 Injuries over the past 5 yrs. • 29 ankle, 6 foot (for 35 injuries) • 22 knee • 12, elbow 36 shoulder 34 wrist (82 UE) • 13 hand, and 7 clavicle
Training and Misc • WGM Self Fulfilling • Even before this many elite coaches predict age 16 as peak. • Men no stats for peak, but most agree it is in the late 20’s. • Time to push and push hard. • We now have foam pits in the world of gymnastics but this means more reps. • Safe reps?
How do we see these injuries • Landing in a hyperdorsiflexed position. • FX 31.1% of the injuries in NCAA ISS • V 27.3% for a combined total of 58.4%. • Warm up, cool down, S&C, other, UB, Beam • Skills • Mostly large skills... • Mostly backwards skills. • Double backflip (tucked, piked, laid out) • Full-in, full-out, double-double, triple double.
Gymnastics Explained • Need large skills for points (to reach a 10.0 for WGM or to increase D Score for MGM) • A-E skills • Do backwards because it is easier to spot landings and more consistent. • Women have to do one forward skill and that’s all they usually do. • Men can do 1/2’s so you end up rolling out. • Unfortunately lots of power to rotate twice and lots of force clanding 5.0x body weight at take-offs and 17.5x BW at landings • McNitt-Gray J • Same goes for vaulting
Other Problem Events • Vault! • Dismounts on Men’s Pbars • All other dismounting events • Not so much for twisting activities even for back twisting
Treatment • Acute Treatment • Follow impingement tx’s of shoulder • Bring down during inflammatory phase • RICE and protect from activity. • ROM Wall stretches, kneeling stretches, • Toes under, toes out. • Strengthening.
Chronic Treatment • Bring down during the inflammphase • Strengthening • Assist in plantarflexionanything • SL Squats • B Heel raise • Step up plus • Weighted bounces • Toe Walks • Eccentric heel raises • Intrinsics to take up the load • Marbles • J’s • Towel Scrunches • Arch-ups • Knee and Hip • Candle stick jumps ups • lunge jump • Box jumps • Fails SL
Rehab • All conservative rehab is stretching and strengthening –Jackie Alvis • We haven’t mentioned any stretching. Mechanical problem
Textbook Orthopaedic Recommendations • Orthopaedic recommendations are “appropriately placed injections or heel lifts” • Dry needling with injection of steroid and local anesthetic can be performed under ultrasound guidance allowing a return to previous levels of activity even in elite athletes, but this technique has not been evaluated in the literature
Goals • Avoid Landing Short! • Extra power at take off • extra absorption of forces at landing • Landing technique • rolling fails • twisting fails • fwd landing/backwards landing
Gymnastics Tricks of the Trade • Appearance must be uniform • 30 seconds for injury or blood • beam and bars • Taping no rules • Appearance should be uniform • Cover ccoflex • Posterior track straps • place in plantar flexion • Elastikon • theraband • Anterior limits • Fxand vault events tennis ball in the front of the ankle. • UCLA team NCAA champs 2010
Surgery • Do they all need them? • No. • Fwd skills • no pain cADL’s • modify gym to avoid over rotation c forward skills • Some do. • limited function out of the gym • failed conservative treatment • Surgical treatment for more resistant cases has a low complication rate and a high level of success. • The previously unsuccessful results of nonoperative treatment for impingement are well recognized in the literature. • Van Dijk reported 62 patients with anterior ankle impingement who did not respond to nonoperative treatment and thus underwent surgery. • Ferkel also reported symptoms of impingement as unresponsive to nonoperativetreatment
Surgery • Bilateral scopes for the last three cases on the gym teams • Walking right away • 4-6 wks of conservative rehab. • 8-10 wks before return to sport • from ROM, open chain, closed chain, NM/perturbation, plyos, return to sport.
Rehab Protocols • Postoperative management involves a compression bandage and partial weight bearing for 3 to 5 days. Patients are instructed to actively dorsiflex. • After surgery the patient was asked to be non-weightbearingfor 2 days to prevent fistula formation through the portal incisions and to allow the soft tissues to settle. • Ankle pumps were encouraged the day after surgery for 20 minutes daily. • After 2 days, instruction was given to increase weight bearing as tolerated. • A postoperative AMI view radiograph was obtained at suture removal to once again assess the removal of the osseous impingement. The soft tissue aspect of AMI was evaluated clinically by pressing in the medial soft spot and dorsiflexing the ankle joint at final follow-up. • Physical therapy was commenced 1 week to 10 days after surgery once the sutures were removed.
Rehab Protocols • Patients discharged from hospital same day with a posterior splint. Non-weightbearing for 5 days. Treated w/ anti-inflammatory meds for 6 wks and postoperative physiotherapy consisting of early passive and active ROM and strengthening exercises, proprioceptive training, and functional exercises specific to dance technique.
Surgical Results • From the late 1980s, several authors have published retrospective studies on management of anterior ankle impingement. Good/excellent results varied between 57% and 67%, with an overall complication rate from 10% to 15%. • 90% of those without joint space narrowing had good or excellent results • van Dijk 1997 • 15 soft tissue impingement and 14 anterior bony impingement cases out of a 79 ankle series. • Amendola 1996
Recurrence? • Coull and colleagues reported recurrence of osteophytes in all their 27 patients who underwent open debridement. • Coull 2003 • At follow-up, most ankles in which osteophytes had recurred were asymptomatic. It is not the osteophyte itself that is painful but the compression of the synovial fold or fibrotic (scar) tissue causes pain. • van Dijk 2001 • 1/11 Reccurence in elite dancers. 9 years following initial surgery. • Nihal2005. • Patients who had osteophytes without joint space narrowing (grade I, 82% good/excellent results) showed significantly better results than did patients who had joint space narrowing (grade II, 50% good/excellent results; • 20/30 Recurrent exostoses in 5-8 years • Tol2006
Surgery • This has allowed grade B recommendations for the use of ankle arthroscopy for the treatment of ankle impingement • Grading and Assigning a Category of Recommendation for Summaries or Reviews of Orthopaedic Studies • A Good evidence (Level I studies with consistent findings) for or against recommending intervention • B Fair evidence (Level II or III studies with consistent findings) for or against recommending intervention • C Poor-quality evidence (Level IV or V studies with consistent findings) for or against recommending intervention • I Insufficient or conflicting evidence not allowing • Glazebrook 2009
Summary • Anterior ankle impingement is relatively common in gymnasts • There are some conservative treatments that can be used • Surgery is effective in treating this condition • Rehabilitation is relatively straight forward
Questions • Questions? • Comments? • Concerns?