Managing a Patient with Abnormal Behaviour: Clinical Approach and Treatment Strategies
300 likes | 402 Vues
Learn how to approach a patient exhibiting abnormal behavior in an emergency setting, differentiate organic vs. functional causes, perform mental status exams, manage restraint effectively, and consider underlying medical conditions. Understand the importance of thorough assessment and intervention in cases of abnormal behavior. Developed by Dr. LP Leung and revised by Dr. Li Yu Kwan in October 2013.

Managing a Patient with Abnormal Behaviour: Clinical Approach and Treatment Strategies
E N D
Presentation Transcript
HKCEM College Tutorial A patient with abnormal behaviour Author Dr. LP Leungrevised by Dr. Li Yu Kwan Oct., 2013
History at Triage • A middle aged man is brought in by police because of exhibiting abnormal behaviour in street. • Personal background unknown • BP (refused) P 100/min • Afebrile (tympanic)
Aims • to identify any immediate life threats • to deal with any disruptive behaviour e.g. aggression • to search for any treatable medical causes • to differentiate organic vs functional conditions • to arrange proper disposal
Treatable medical causes • Drug effect • Metabolic disorders • Endocrine causes • Nutritional causes • Trauma and tumor • Infection • Atherosclerotic complications
Mental State Examination • Appearance: dress, hygiene… • Sensorium: orientation, memory, LOC… • Speech: fast, slow, slur • Emotion: mood and affect • Thought: process, content, delusion • Perception: hallucination, illusion • Attitude = rapport, insight
Further observations • He is around 40 years old. • Dressed properly and clean. • He is speaking fast, talking to air at times. • Elated and attempted to PU in front of you. • Afebrile, vital signs all normal. • Physical exam incomplete since patient is not cooperative • Any stat investigation? H’stix = 5 mmol/L
Ddx • Alcohol or drugs • endocrine e.g. hyperthyroidism • infections esp of CNS • trauma • psychiatric e.g. mania • post-ictal
How would you differentiate organic / functional causes in general ? History Physical exam MSE Lab investigations
History • Course : first episode >> organic • Onset : sudden >> organic • Past hx : medical / psychiatric • Drugs
P/E • Age > 40 yr >>> organic • abnormal vital signs, including conscious level • focal neurological signs / symptoms
MSE • Organic • labile mood • visual , somatic, olfactory hallucinations • recent memory impaired • disoriented • attends occasionally • Fluctuating conscious state • Functional • blunted affect • auditory hallucination • remote memory impaired • oriented • unable to attend • Stable conscious state
He is becoming more and more elated and starts to disturb others.What is your approach to control him ?
Approach • Ensure your own safety first • attempt to talk down patient, though this is usually not effective • consider restraint, physical or chemical or both
Drugs • Neuroleptic : • drug of choice > haloperidol IMI • Benzodiazepine : • drug of choice : lorazepam or midazolam IMI / IVI
How would you perform physical restraint? • Who? • When? • How?
aspiration Physical restraint • Team approach • 5 persons with one act as leader • Leader: head and trunk • Each will hold one limb • Documentation + monitoring essential How may a patient die in restraint?
Remember to document • The reason to restrain • Time of application and the intended duration • Expected time of review • Type of restraint device • Discussion/explanation with patient and/or family members • Regular monitor of vital signs, state of circulation
Complications of physical restraint • Bruises and Abrasions • Circulatory compromise • Immobilization cause pressure sores, paresthesias • Aspiration • Suffocation especially in the prone position • Protracted struggling vs restraint cause hyperthermia, lactic acidosis, rhabdomyolysis
While the nurses attempt to restrain him, he develops a generalized seizure which lasts for 30 sec..
Apart from the standard emergency tx of seizure, any Ix would you consider in the A&E setting ?
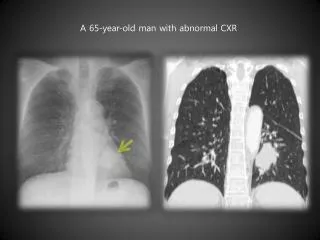
Urgent Ix • Repeat Glucose • electrolytes • ABG • drug profile • CBP, LRFT, TFT, culture • ECG • CT brain (plain)
He is admitted and CT brain shows a frontal lobe tumor .On review, his behavior is due to disinhibition caused by the tumor.
You should be aware : • Abnormal behavior is not equivalent to psychiatric illness. • Psychiatric illness is in fact a dx of exclusion in ED. • Physcial exam is often incomplete since patient is not cooperative. • High risk factors for organic causes : • the young and old • first episode • acute onset • abn. vital signs incl. Altered consciousness
Reference • HAHO guideline for the use of physical restraint (2008) • Physical and Chemical Restraints. Emerg Med Clin N Am 27(2009) 655-667