Download
1 / 27
300 likes | 404 Vues
BIOLOGICAL HAZARDS IN HEALTH CARE FACILITIES. Chr. Papazoglou, G. Dounias , V. Makropoulos Department of Occupational & Industrial Hygiene National School of Public Health (NSPH). Background.

E N D
BIOLOGICAL HAZARDS IN HEALTH CARE FACILITIES Chr. Papazoglou, G. Dounias, V. Makropoulos Department of Occupational & Industrial Hygiene National School of Public Health (NSPH)
Background More people are employed in the health care sector than in any other industry p.e. in USA.Health care workers [HCWs] are at occupational risk for a vast array of infections that cause substantial illness and occasional deaths. Despite this, few studies have examined the incidence, prevalence, or exposure-associated rates of infection or have considered infection-specific interventions recommended to maintain worker safety.
Historical Overview • Hippocrates “…ο μεν γαρ ιητρός ορή τε δεινά, θιγγάνει τε αηδέων, επ' αλλοτρίησί τε ξυμφορήσιν ιδίας καρπούται λύπας…" (Ιπποκράτης, Περί Φυσών - 1). • HCW are obligate to treat patients who may be contagious. • Galen fled at the height of the Roman plague. • In other outbreaks, physicians who could not flee did the next best thing: They "locked themselves into their houses and refused to come out". • Cities responded by hiring "plague doctors" who, in exchange for salary, home, and citizenship, stayed behind to treat the infected. • Other illnesses similarly failed to inspire the heroic among HCWs. Valsalva, Morgagni, and Laennec refused to do autopsies of those dying of tuberculosis for fear of catching the disease (a justifiable concern; Laennec, among many other physicians, was destined to die of tuberculosis). • Ramazzini as “medico condotto” near Viterbo was infected by malaria [occupdisease ?!] • Early 20th century, scarlet fever and diphtheria comprised half of all infections treated in hospitals, and as many as 5% of staff members contracted these diseases as a result of occupational exposure. Infection control interventions, including gauze masks for scarlet fever and vaccination for diphtheria, successfully controlled the problem. • In 1847, a Code of Ethics written by the fledgling AMA declared it the physician's duty to "face the danger" of caring for the contagious even "at jeopardy of their own lives". • A 1957 revision of the Code, however, not only deleted this section but asserted the physician's right to be "free to choose whom to serve," suggesting that refusal to provide care was acceptable.
Occupationally Acquired Infections Encountered in Specific Groups of Health Care Workers*[Kent A. Sepkowitz]
health care workers who die of occupationally acquired illnesses receive little public attention! • Despite this recognized risk, no country has a system in place to track fatal, occupationally acquired infections in their entirety.
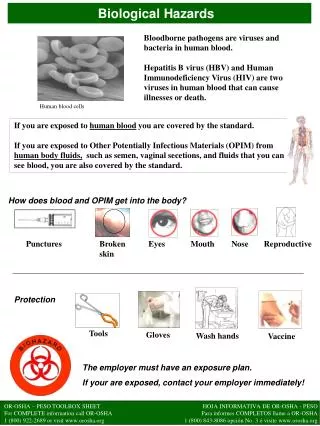
Biological Hazards Bacteria-Tetanus,Tuberculosis, Anthrax, Brucellosis (Milkmen),Gonorrhea(Sex-workers-Genital organs get affected). Virus - Hepatitis, AIDS Protozoal&Parasitic-Malaria,Hydatid(Dog handlers),Hookworms, tapeworms (Agri-workers), etc. Fungi-(Agri-workers)-Tinea-infections, Coccidiomycosis, Psittacoses, ornithosis, etc.
Data Synthesis • Occupational transmission to HCWs was identified for numerous diseases, including infections caused by • bloodborne organisms (HIV, HBV, HCV, CMV, Ebola virus), • organisms spread through the oral-fecal route (salmonella, HAV), and • organisms spread through direct contact (HSV, Sarcoptes scabiei).
Occupationally Acquired Infections Resulting from Bloodborne Transmission* Sepkowitz, K. A. Ann Intern Med 1996;125:917-928
Occupational Diseasesin Europe • Infectious diseases Health and social work and public administration covered the majority of cases of Hepatitis C (97%), Hepatitis A (88%), tuberculosis (88%) and Hepatitis B (60%).
HCV (+)HCWsin Europe0,2-3% J Clin Virol 2003: 27: 213-230,
HBsAg(+) [0,3-3%]& ΑΝΤΙ-HBc (+)[4-30%]HCWsin Europe J Clin Virol 2003: 27: 213-230
Occupational Infection Diseases in Greece • IKA, the largest Social Security Organisation in Greece. It covers 5,530,000 workers and employees and provides 830,000 pensioners with retirement pension.IKA covers those in dependent employment in Greece or abroad for an employer who is based in Greece, as well as those who offer full-time or part-time personal labour on commissioned work agreements and are not insured with any other main insurance agency. IKA also covers certain groups of people who offer their labour to various employers at various times and whose insurance is realized through their Unions or Insurance Associations, (e.g. porters, news-stand vendors, slaughterhouse workers etc.) or through special provisions (e.g. exclusive nurses). • K.A. art.40 • Anghylostoma, • Anthrax, • Brucellosis, • Hepatitis B, • Leptospirosis • TBc, • Tetanus.
Occupational bio hazards: Novel risk factors • Novel viruses and prions, emerging in different parts of the world, may pose a particular threat to health and life of HCWs, agriculture workers and veterinarians. A new coronavirus (SCoV) that evoked a rapid outbreak of disease described as severe acute respiratory syndrome (SARS) in the first half of 2003 may serve as an example. The disease was particularly common among HCWs. • Previously discovered zoonotic viruses, Nipah virus in pigs and Hendra virus in horses, may be a cause of fatal encephalitis in animal farmers. Hantaviruses (Puumala, Hantaan, Sin Nombre and others) infecting field rodents may be a cause of hemorrhagic fever with renal syndrome (HFRS) or pulmonary syndrome (HPS) in farmers and laboratory workers. Prions responsible for inducing a zoonotic variant of Creutzfeldt-Jakob disease (vCJD) are considered to be a potential cause of work-related infections in agricultural and HCWs, however, this assumption has not as yet been supported by any conclusive evidence. • In many countries, blood-borne occupational infections with HCV is the major epidemiological problem among HCWs, mostly because no vaccine against this virus has been produced to date. Vaccinations effectively restricted the number of occupational infections with HBV, and work-related infections with HIV causing AIDS are very rare.
TLVs of occupational exposure to bioaerosols • Occupational biohazards include not only factors that have long been known (viruses, bacteria, fungi, parasites), but also agents exerting allergic and toxic effects, which are directly responsible for the development of various diseases in many occupational groups. • Numerous agents of this group (allergens, microbial toxins, pollen allergens and allergens of animal origin) are components of bioacrosols--potential hazards inducing occupational respiratory diseases among farmers and people involved in other occupations. • Contrary to the majority of chemical and physical factors, neither commonly approved criteria for assessing exposure to biological factors, nor threshold values and methodological recommendations are as yet available. The lack of these criteria renders it difficult to implement in many countries [Directive 2000/54/EC ]. • TLVs of occupational exposure to bioaerosols associated with plant and animal dusts, including: mesophilic bacteria, Gram-negative bacteria, thermophilic actinomycetes, fungi and bacterial endotoxins. The Institute of Rural Medicine in Lublin proposals could be considered as a starting point for developing appropriate facultative standards that would facilitate the practical implementation of the aforesaid Directive. Meantime it is essential to be strict in following the binding concentration limits of the plant and animal dusts in the air.
Most outbreak-associated attack rates range from 15% to 40%. Occupational transmission is usually associated with violation of one or more of three basic principles of infection control: • handwashing, • vaccination of HCWs, and • prompt placement of infectious patients into appropriate isolation.
protection of HCWs • existing national legislative frame compared to international experience (WHO, ICOH, SMLII, ACOEM). • Small number of Occupational Physicians in NHS in Greece. • No OccupHealthServices
Primary prevention of exposures, as recommended by universal precautions guidelines, remains the cornerstone of protecting healthcare workers. Nonetheless, a substantial number of parenteral exposures continue to occur. Updated developments and recommendations for the protection of HCWs from bloodborne pathogens are provided. • The predominant evidence suggests that total percutaneous injuries have decreased over the last decade. Thoughtful adherence to universal precautions remains the primary means of preventing occupational exposures and thus of reducing occupational risk of infection with bloodborne pathogens. • A number of studies have provided additional evidence for the efficacy of safety devices in reducing specific subsets of injuries when combined with education and administrative interventions. Barriers to and positive predictors of universal precautions compliance have been identified. • Postexposure prophylaxis [PEP] remains the second line of defense; several authorities have now recommended three antiretroviral agents in this setting.
Postexposure prophylaxis (PEP) • Recommendations for HBV PEP management include initiation of the HB vaccine series to any susceptible, unvaccinated person who sustains an occupational blood or body fluid exposure. PEP with hepatitis B immune globulin (HBIG) and/or HBV series should be considered for occupational exposures after evaluation of the HBsAg status of the source and the vaccination and vaccine-response status of the exposed person. Guidance is provided to clinicians and exposed HCWs for selecting the appropriate HBV PEP. • Immune globulin and antiviral agents (e.g., interferon with or without ribavirin) are not recommended for PEP of hepatitis C. For HCV PEP management, the HCV status of the source and the exposed person should be determined, and for HCWs exposed to an HCV positive source, follow-up HCV testing should be performed to determine if infection develops. • Recommendations for HIV PEP include a basic 4-week regimen of two drugs (zidovudine and lamivudine; 3TC and stavudine ; or didanosine and d4T) for most HIV exposures and an expanded regimen that includes the addition of a third drug for HIV exposures that pose an increased risk for transmission. When the source person's virus is known or suspected to be resistant to one or more of the drugs considered for the PEP regimen, the selection of drugs to which the source person's virus is unlikely to be resistant is recommended.
Postexposure prophylaxis (PEP) • In addition, in several special circumstances (e.g., delayed exposure report, unknown source person, pregnancy in the exposed person, resistance of the source virus to antiretroviral agents, or toxicity of the PEP regimen) when consultation with local and/or the NHS experts is advised. • Occupational exposures should be considered urgent medical concerns to ensure timely postexposure management and administration of HBIG, hepatitis B vaccine, and/or HIV PEP.
Integrated comprehensive occupational surveillance system for HCWs. • Human resources job and work location data used to define population at risk. • Outcomes and exposure data from existing occupational health and safety programs, health promotion programs, and employee health insurance claims, linked with human resources data and de-identified to create the Health and Safety Surveillance System (HSSS).
In summary • daily patient care presents a real, although small, risk for infection for HCWs. • Indeed, the cost to prevent, control, and treat occupationally acquired infections is considerable, in terms of both money spent and lives affected. • This does not imply that working with contagious persons is a heroic endeavor.
In summary • Vaccines, • effective infection control procedures, • safer procedures, and safer devices will all be necessary, • along with a better understanding of factors that influence HCWs behaviors that result in injury. • In addition, a number of issues relating to the postexposure management of occupational exposures with bloodborne pathogens need to be better understood.