Download
1 / 19
190 likes | 288 Vues
Learn about concussion symptoms, signs, types, and management protocols in sports. Understand the importance of proper evaluation, rest, and monitoring for a safe return to play after a concussion.

E N D
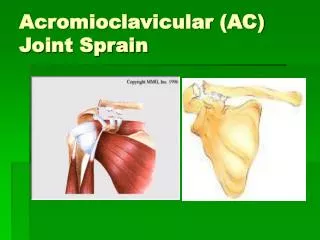
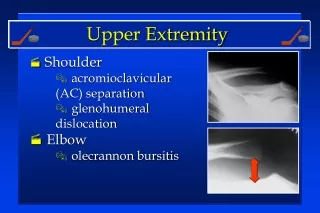
Upper Extremity • Shoulder • acromioclavicular (AC) separation • glenohumeral dislocation • Elbow • olecrannon bursitis
Upper Extremity • Wrist • distal radius fracture • scaphoid (navicular) fracture • ECU (tendon) subluxation/dislocation • DRUJ (ligament) sprain
Upper Extremity • Hand • ulnar collateral (thumb ligament) sprain • phalanx (finger) fracture
Lower Extremity • Abdomen/Groin/Hip • athletic pubalgia • adductor (groin) strain • iliopsoas/rectus (hip flexor) strain
Lower Extremity • Knee • MCL sprain • ACL sprain • quadriceps contusion
Lower Extremity • Ankle • malleolar bursitis • distal fibula fracture • syndesmosis/lateral ligamentsprain
Lower Extremity • Foot • contusion/fracture • calcaneal bursitis
Catastrophic Injuries • Traumatic Brain Injury • (Concussion) • Cervical Spine Fracture/Dislocation • (± spinal cord injury) • Eye Injuries
Catastrophic Injuries • Upper Airway • (larynx, hyoid, soft tissues) • Commotio Cordis • (chest blow) • Subarachnoid Hemorrhage • (neck blow) • Spleen Rupture • Neck Laceration
Concussion Concussion may be caused by a direct blow to the head, face, neck or elsewhere on the body that results in an impulsive force transmitted to the head causing a rapid onset of short-lived impairment of neurologic function that resolves spontaneously.
Concussion Symptoms: unaware of situation, confusion, amnesia, loss of consciousness, headache dizziness, nausea, loss of balance, flashing lights, ear ringing, double vision, sleepiness, feeling dazed
Concussion Signs: altered mental status, poor coordination, seizure, slow to answer, poor concentration, nausea, vomiting, vacant stare, slurred speech, personality changes, inappropriate emotions, abnormal behavior
Concussion • repeated concussions cause cumulative damage increased severity with each incident • initial concussion chance of a 2ndconcussion is 4x greater
Simple Concussion • Progressively resolves without complication over 7-10 days: • all concussions mandate evaluation by physician • limit training & competition while symptomatic • able to resume sport without further problems • managed by certified athletic trainers working under medical supervision • formal neuropsychological testing unnecessary?
Complex Concussion • Specific features, persistent symptoms or recurrence with exertion: • prolonged loss of consciousness (>1 minute) • multiple concussions over time • repeated concussions with less impact force • neuropsychological testing helpful • multidisciplinary management • (experienced sports medicine physician, sports neurologist or neurosurgeon, neuropsychologist)
Concussion Management A player with ANY symptoms or signs: • should not be allowed to return to play in the current game or practice • should not be left alone- regular monitoring for deterioration is essential • should be medically evaluated following the injury
Concussion Management Return to play must follow a medically supervised stepwise process: • monitored by a medical doctor • player should never return to play while symptomatic “When in doubt, sit them out!”
Concussion Management • physical andcognitive rest • monitoring of: • symptoms • neurocognitive function • postural stability • neuropsychological testing (?) • graded exertion protocol
Concussion Management • Return to Play Protocol • 1. No activity, complete rest • 2. Light aerobic activity (walking, stationary cycling) • 3. Sports specific training- skating. • 4. Non-contact training drills • 5. Full-contact training after medical clearance • 6. Return to competition • * Proceed to the next level only if asymptomatic • * Any symptoms or signs: drop back to the previous level & attempt progression again after 24 hours