Standard 11 Transfusion Guidelines
Standard 11 Transfusion Guidelines. Irwin Gross, M.D. Medical Director Patient Blood Management Eastern Maine Medical Center. A little about Eastern Maine Medical Center. 400 bed community and tertiary care hospital in rural Maine Large hospitalist service High risk obstetrics

Standard 11 Transfusion Guidelines
E N D
Presentation Transcript
Standard 11Transfusion Guidelines Irwin Gross, M.D. Medical Director Patient Blood Management Eastern Maine Medical Center
A little about Eastern Maine Medical Center • 400 bed community and tertiary care hospital in rural Maine • Large hospitalist service • High risk obstetrics • Trauma center, Level 2 • Dialysis center • Family Practice residency • Cardiac surgery program • Approx. 450 cases/yr. • Active heme/onc service • 10 oncologists • No transplant surgery
There is effective implementation of comprehensive, written evidence-based guidelines for transfusion of blood components Effective implementation
Who should develop the guidelines? Should the guidelines be mandatory? Why the Medical Executive Committee?
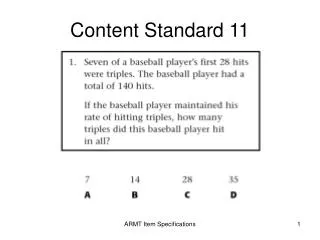
What is the difference between prospective, concurrent and retrospective review? Which is most effective? Easiest? Hardest? Who should do the review? How do determine medical appropriateness? How do you know if review is effective?
Evaluating the Impact of Peer Review Process vs. Outcome Metrics • Measure impact of peer review • Many committees use process metrics • Process metric: a metric that measures if a goal-directed activity performed • Examples of process metrics: • Number of transfusions with a letter to the provider with copy to Department Chair • Number of transfusions deemed clinically inappropriate by committee • These metrics can be misleading • Hard to compare to other hospitals • May not tell you anything about clinical outcomes • Fewer letters may mean less rigorous review, not better transfusion practice Move away from metrics that look at committee activities
Evaluating the Impact of Peer Review Process vs. Outcome Metrics • Outcome measures preferred over process measures • Measures the result of a goal - directed activity, function or process (processes you implemented to change transfusion practice) • Examples: • average pre-transfusion hemoglobin overall and by provider • average number of units transfused per patient by DRG • percentage of inpatients transfused • Number of transfusions with post-transfusion hemoglobin above 10 g/dl
How do you communicate the results of transfusion review? How would that be different for prospective review vs. concurrent vs. retrospective? What type of transfusion review might be shared besides individual transfusion episodes?
Reporting the Data • Types of reports • Service specific reports • Provider specific reports • Provider “report cards” • Diagnosis / procedure specific reports • Can report by provider • Global reports and trending data • Program “report cards”
Transfusion “Report Cards”Exception Reporting Pre-transfusion Hgb
How do you make the guidelines available in your hospital? Are they available to the ordering physician at the time they make a transfusion decision? How do you ensure that the ordering provider DOES look at transfusion guidelines. Are the guidelines incorporated into your order sets or CPOE process?
Electronic Tools to Facilitate Transfusion Peer Review Computerized Physician Order Entry (CPOE) enhances ability to review individual transfusions • All transfusions captured electronically • Indication captured if part of order • Time, basic lab data captured • 100% accuracy re: ordering physician • Report can be developed to flag transfusions for review Dzik, Transfusion 2007;47:142S-144S
Why is it important that the guidelines incorporate information other than just “transfusion triggers” What information is included as part of your guidelines? Is it objective or subjective information? At transfusion committee, are the patient specific factors applied objectively so that committee members aren’t simply “justifying” any and all transfusion decisions as appropriate based on “clinical judgment.”
How often do you review your guidelines? What do you use as an evidence base for guideline review? Do you use guidelines from other institutions and organizations? How do you ensure that your guidelines are consistent with the literature and evolving standard of care?
ADULT ANEMIA – ACTIVELY BLEEDING INDICATIONS: • Note: Blood Volume is 70 mL/kg in adults. • Acute loss of blood greater than 25% of blood volume unresponsive to fluid resuscitation. • Acute loss of blood and Hgb less than 8.5 gm/dL (Hct 25%) and documented moderate or severe ischemic heart disease. • Fall in Hgb of 2 gm/dL (Hct of 6%) within 24 hours AND Hgb less than 8 gm/dL (Hct 24%) AND signs/symptoms of anemia or tissue hypoxia (Tachycardia, hypotension, or mixed venous oxygen saturation less than 55% unresponsive to other measures). • ADULT ANEMIA – NOT ACTIVELY BLEEDING INDICATIONS: • Note: Optimize hemodynamics and oxygenation before considering transfusion. • Hgb less than 6 gm/dL without expected response to medical therapy. • Pre-operative Hgb less than or equal to 7 gm/dL (Hct 21%) when alternative therapy (e.g. B12, Folate, IV Iron, Erythropoietin) is not appropriate or sufficient. • Post-operative Hgb less than 7 gm/dL AND signs/symptoms of anemia or tissue hypoxia1. • Hgb less than or equal to 7 gm/dL (Hct 21%) AND signs/symptoms of anemia or tissue hypoxia1 without expected response to medical therapy. • Hgb less than or equal to 7 gm/dL (Hct 21%) in a patient with stable ischemic heart disease AND signs/symptoms of anemia or tissue hypoxia. • Hgb less than or equal to 8 gm/dL (Hct 24%) AND acute coronary syndrome with signs/symptoms of anemia or clinical evidence of myocardial ischemia2. • Hgb less than 7 gm/dL in patient receiving chemotherapy or radiotherapy. • Hgb less the 8 gm/dL in patient with traumatic brain injury and/or intracranial hypertension. • Hgb less the 8 gm/dL and chronic transfusion regimen for Thalassemia, Myelodysplasia, primary marrow disorder, or other red cell disorder. • 1 Signs/symptoms of anemia and/or tissue hypoxia are tachycardia, hypotension, new EKG changes, • mixed venous oxygen saturation less than 55%, or clinical evidence of myocardial ischemia. • 2 Signs/symptoms of myocardial ischemia are recurrent chest pain, active heart failure, or syncope.