Brachial Plexus Block Above the Clavicle
720 likes | 2.29k Vues
Brachial Plexus Block Above the Clavicle. Edited by Dr. M Dorgham Under supervision of Proff Dr. Amr Abdelfattah. Objectives. Review the Anatomy of brachial plexus. Neurostimulation guided approaches . Sonoanatomy and Ultrasound guidance . Complications

Brachial Plexus Block Above the Clavicle
E N D
Presentation Transcript
Brachial Plexus Block Above the Clavicle Edited by Dr. M Dorgham Under supervision of Proff Dr. Amr Abdelfattah
Objectives Review the Anatomy of brachial plexus Neurostimulation guided approaches Sonoanatomy and Ultrasound guidance Complications Advantages of ultrasound guidance
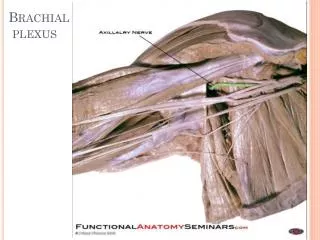
Anatomy of Brachial Plexus • The brachial plexus is a network of nerve fibers , running from the spine, formed by the ventral rami of the lower four cervical and first thoracic nerve roots (C5-T1). It proceeds through the neck, the axilla (armpit region), and into the arm. • The brachial plexus is responsible for cutaneous and muscular innervation of the entire upper limb, with two exceptions: • The trapezius muscle innervated by the spinal accessory nerve (CN XI) and • An area of skin near the axilla innervated by the intercostobrachial nerve.
Anatomy of Brachial Plexus The brachial plexus is divided into Roots Trunks Devisions Cords Branches
INTERSCALENE BLOCK ANTERIOR APPROACH
Superficial anatomy The sternal head of the sternocleidomastoid muscle (1) is anterior to its clavicular head (2), which forms the anterior border of the posterior triangle of the neck. The accessory nerve (3) is superficial to the fascial floor of the posterior triangle of the neck and originates close to the lesser occipital nerve (4). The superficial cervical plexus (5) is superficial to the fascial floor of the posterior triangle of the neck and gives rise to the supraclavicular nerves (6). The superficial cervical plexus originates from C2 and supplies the ipsilateral skin of the neck, shoulder and occipital area with sensory fibers. The trapezius muscle (7) is innervated by the accessory nerve (3), and the nerve to levator scapulae innervates the levator scapulae muscle (8).
Deeper anatomy A view of the anatomy with the sternocleidomastoid muscle removed shows the position of the internal jugular vein (1) (cut off here). Deep to the internal jugular vein is the thoracic duct (2) on the left side of the neck and adjacent to that the Anterior scalene muscle (3). Posterior to that is the middle scalene muscle (4) and more posterior, the posterior scalene muscle (5). Posterior to the posterior scalene muscle is the levator scapulae muscle (6) with the nerve to the levator scapulae muscle (7). The accessory nerve (8) as well as the trapezius muscle (9) can be seen. Also note the vagus nerve (10), which is situated in close relationship to the carotid artery (11), and the phrenic nerve (12), which is situated on the belly of the anterior scalene muscle (3). The brachial plexus (13) is situated between the anterior and middle scalene muscles. The suprascapular nerve (14) and the dorsal scapular nerve (15) (which innervates the rhomboid muscles) branches from the brachial plexus. Note that the subclavian artery (16) lies anterior to the brachial plexus.
Surface anatomy 1 = Phrenic nerve 2 = Brachial plexus 3 = Dorsal scapular nerve (to rhomboid muscles) 4 = Nerve to levator scapulae
POSTERIOR APPROACH (OR CONTINUOUS CERVICAL PARAVERTEBRAL BLOCK) The continuous cervical paravertebral block is ideal for relief of postoperative pain following shoulder surgery, especially arthroscopic shoulder surgery. This approach sometimes does not involve the nerves of the superficial cervical plexus and the skin around the shoulder area will therefore not be anesthetized. Although not yet evaluated by formal research, the experience of this author is that loss of resistance to air as well as nerve stimulation may be used for the placement in this block. If proven successful, this should make this block ideally suited for postoperative use, and when severely painful conditions such as fractures of the shoulder are present where nerve stimulation is not advisable or impractical.
Anatomy The brachial plexus (1) is situated between the anterior (2) andmiddle (3) scalene muscles, while the vertebral artery (4) is guarded by the bony structures of the vertebrae. The posterior approach for ISB is antero-lateral to the trapezius muscle (5) and postero-medial to the levator scapulae muscle (6).
Anatomy The point of needle entry is in the apex of the “V” formed by the trapezius muscle posterior and the levator scapulae muscle anterior – the “B”-spot
Surface anatomy Needle entry should be at the level of C6 and just antero-lateral to the trapezius muscle and postero-medial to the levator scapulae muscle in the apex of the “V” formed by these two muscles.
Needle placement The nerve stimulator is clipped to the needle and a loss-of-resistance to air device is placed on the needle. The needle is directed , anteriorly and caudad, aiming for the suprasternal notch. The needle is carefully “walked off” the transverse process of C6 and loss of resistance to air and muscle twitches of the shoulder girdle appear simultaneously.
Ultrasound guided Interscalene Brachial plexus block
The patient is in semi-sitting supine position with the head facing away from the side to be anesthetized. The premedication of an adult, average size patient typically consists of 2-4 mg of midazolam; 250mcg -500mcg of alfentanyl administered just before insertion of the needle TIP:Visualization of the brachial plexus in the interscalene grove can be challenging in patients who are tense, moving or exhibit guarding. Proper sedation can go a long way toward obtaining quality images.
The ultrasound probe (10-12MHz) is applied in the axial oblique plane closer to the midline and angled to first visualize the carotid artery
Note the position of the internal jugular vein (IJ) as the pressure on the ultrasound probe is lightened. The internal jugular vein is positioned slightly superficially and lateral to the carotid artery. Changing the pressure on the probe causes the IJ to open and close.
The ultrasound probe is then moved slightly laterally to visualize the brachial plexus in the interscalene grove between anterior and middle scalene muscles. The roots/trunks (N) of the brachial plexus are seen stacked between the scalene muscles usually as round, hypoechoic structures
Sliding or angling the ultrasound probe slightly more inferior allows visualization in the low-interscalene position in which the brachial plexus is positioned in proximity to the subclavian artery
After the brachial plexus is identified on the image, a 50 mm (max) stimulating needle is inserted perpendicular to the long axis of the ultrasound probe. The needle is inserted at the point on the probe that corresponds to the location of the brachial plexus on the screen The needle insertion results in shadowing of the ultrasound image which indicates the path of the needle TIP: Make sure to estimate the exact depth of the brachial plexus (typically 0.5-1.5 cm) before inserting the needle. The needle should never be inserted deeper than the depth indicated on the ultrasound image.
Injection of local anesthetic is made with monitoring of the dispersion of the injectate. If the injectate does not appear to fill the lower compartment of the interscalene space, the needle is slightly advanced (0.5-1cm) and additional injection is made at a slightly greater depth (0.5-1cm deeper). Local anesthetic is injected slowly and with frequent aspirations, while avoiding excessive injection pressures (<20 psi). Thirty to forty ml of local anesthetic is more than adequate for reliable blockade of the brachial plexus. Typical indications for this block are surgery on the shoulder, lateral clavicle, acromioclavicular joint, proximal humerus and elbow (with low interscalene block).
Supraclavicular Brachial Plexus Block
The trunks divide behind the clavicle into anterior and posterior divisions, which separate the innervation of the ventral and dorsal halves of the upper limb.
Ultrasound guided Supraclavicular Brachial Plexus Block
POSITIONING • The patient is placed supine • The patient’s head is turned toward the contralateral side • The operator is positioned on the ipsilateral side • The ultrasound machine should be placed on the contralateral side SONOANATOMY. The subclavian artery appears hypoechoic and pulsatile and the individual nerves as hypoechoic small circles. It is very important to identify the pleura while performing this block so as to avoid pneumothorax. The first rib acts as a backstop to prevent pleural puncture, which means that the needle tip is in the same plane
the "chimney" effect as local anesthetic is forced to spread up between the anterior and middle scalene muscles, unable to go down because the first rib is in the way.
Pre injection Post injection
The major advantage of the supraclavicular approach is that the nerves are very tightly packed, so that the onset is fast and the blockade deep, leading to this technique being nicknamed “the spinal of the arm”. • Ultrasound guidance, the pleura can be visualized, and as long as proper technique is used, i.e. if the needle, and especially the needle tip, is visualized at all times, pneumothorax should not occur. • Typical Indication : For surgeries below the mid-humerus level. It will not diffuse to the lower roots of the cervical plexus, and thus will not block the upper aspect of the shoulder. • Twenty to Forty mls local anaesthetic is adequate for reliable block
Possible Complications • Peripheral Nerve Injury • Most nerve injury presents as residual paresthesia, hand or forearm hypoesthesia, and rarely as permanent Paresis • The overall incidence of long-term nerve injury ranges between 0.02% and 0.4% • Vascular Injury • The risk of hematoma immediately after brachial plexus techniques is small (0.001 to 0.02%) • Muscle Injury • Myonecrosis from local anesthetics at concentrations typically achieved at the site of injection is well proven and characteristic of all local anesthetics, with bupivacaine producing the most intense effect. Because damage is dose related, continuous • local anesthetic administration may worsen injury.
Hemidiaphramatic Paresis • The proximity of the phrenic nerve to the interscalene groove frequently leads to unintended local anesthetic block and resultant diaphragmatic dysfunction. • The incidence of hemidiaphragmatic paresis (HDP) is 50-100% after interscalene brachial plexus block • Pneumothorax • The reported incidence of pneumothorax after supraclavicular block is 0.5% to 6.1% • Intravascular Injection • local anesthetic injected directly into the vertebral or carotid artery, or retrograde flow of local anesthetic via the subclavian artery, may proceed directly to the brain.
Subarachnoid or Epidural Injection. • Interscalene brachial plexus block has been linked to unintended subarachnoid block and to cervical or thoracic epidural block. • Cervical Sympathetic Chain. • Excessive local anesthetic spread can also affect the cervical sympathetic chain, causing the patient to manifest Horner’s syndrome. • with20% to 90% incidence • Recurrent Laryngeal Nerve. • Hoarseness may transpire after interscalene block or after 1.3% of supraclavicular blocks
Advantages of Ultrasound Guidance • Ultrasound guidance with real-time needle visualization in relation to anatomic structures and target nerves makes regional anesthesia safer and more successful. • With ultrasound guidance in experienced hands, brachial plexus blockade can lead to • Decreased block performance and onset time, • Increased success rate and • Decreased rate of complications. • These advantages result in increased operating room efficiency, as well as increased patient satisfaction.
The infraclavicular block is a blockade of the brachial plexus below the level of the clavicle and in the proximity of the coracoid process. This block is uniquely well-suited for hand, wrist, elbow, and distal arm surgery. It also provides excellent analgesia for an arm tourniquet. As opposed to a supraclavicular block, an infraclavicular block is not a good choice for shoulder surgery.