Download
1 / 23
230 likes | 417 Vues
A Phase III, Randomized, Double-Blind, Placebo-Controlled Registration Trial to Evaluate the Efficacy and Safety of Placebo + Trastuzumab + Docetaxel vs. Pertuzumab + Trastuzumab + Docetaxel in Patients with Previously Untreated HER2-Positive Metastatic Breast Cancer (CLEOPATRA).

E N D
A Phase III, Randomized, Double-Blind, Placebo-Controlled Registration Trial to Evaluate the Efficacy and Safety of Placebo + Trastuzumab + Docetaxel vs.Pertuzumab + Trastuzumab + Docetaxelin Patients with Previously Untreated HER2-Positive Metastatic Breast Cancer (CLEOPATRA) J Baselga, J Cortés, S-B Kim, S-A Im,R Hegg, Y-H Im, L Roman,J L Pedrini, T Pienkowski, A Knott, E Clark, M C. Benyunes, G Ross, and S M Swain 1. Baselgaet al. N Engl J Med 2011
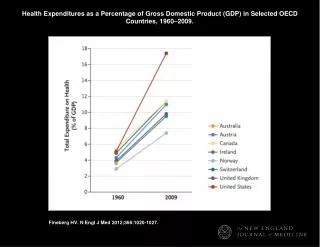
Introduction and study objective 1. Slamonet al. N Engl J Med 2001; 2. Nahta &EstevaOncogene 2007;3. Franklin et al. Cancer Cell 2004; 4. Baselgaet al. J ClinOncol 2010;5. Gianni et al. Cancer Res 2010 Suppl 2; 6. Baselga &Swain Clin Breast Cancer 2010 HER2, human epidermal growth factor receptor 2;MBC, metastatic breast cancer Trastuzumab-based therapy is the current standard of care inHER2-positive MBC1 • However, progression of breast cancer still occurs in a majority of patients2 Pertuzumab is a humanized monoclonal antibody and HER2 dimerization inhibitor that binds HER2 at a different epitope than trastuzumab3 Phase II trials in patients with HER2-positive breast cancer have shown improved activity, and a good safety profile with pertuzumab-trastuzumab-based therapy4,5 CLEOPATRA assessed efficacy and safety of a pertuzumab-trastuzumab-based regimen in first-line treatment of patients with HER2-positive MBC6
Study design PD Placebo + trastuzumab n=406 Docetaxel*≥6 cycles recommended Patients withHER2-positive MBCcentrally confirmed (N=808) 1:1 PD Pertuzumab + trastuzumab n=402 Docetaxel*≥6 cycles recommended • Randomization was stratified by geographic region and prior treatment status (neo/adjuvant chemotherapy received or not) • Study dosing q3w:- Pertuzumab/Placebo: 840 mg loading dose, 420 mg maintenance- Trastuzumab: 8 mg/kg loading dose, 6 mg/kg maintenance - Docetaxel: 75 mg/m2, escalating to 100 mg/m2 if tolerated *<6 cycles allowed for unacceptable toxicity or PD; >6 cycles allowed at investigator discretion MBC, metastatic breast cancer; PD, progressive disease
Key patient eligibility criteria Centrally confirmed HER2-positive (IHC 3+ and/or FISH-positive; ratio ≥2.0) locally recurrent, unresectable, or metastatic breast cancer Measurable and/or non-measurable disease LVEF ≥50% at baseline No more than one hormonal regimen for MBC prior to randomization (Neo)adjuvant systemic breast cancer chemotherapy including trastuzumab and/or taxanes allowed if followed by a disease-free interval of ≥12 months No history of CHF or LVEF decline to <50% during or after prior trastuzumab therapy CHF, congestive heart failure; FISH, fluorescence in situ hybridization; IHC, immunohistochemistry; LVEF, left ventricular ejection fraction;MBC, metastatic breast cancer
Study endpoints Baselgaet al. Clin Breast Cancer 2010. Primary endpoint • Independently assessed progression-free survival (PFS) Secondary endpoints • Overall survival • Objective response rate • Safety • PFS by investigator assessment • Duration of response • Evaluation of biomarkers and correlation with clinical outcomes • Time to symptom progression
Statistics Progression-free survival • 800 patients and ~381 PFS events were required to provide 80% power to detect a 33% improvement in independently assessed PFS(HR = 0.75) at the two-sided significance level of 5% Overall survival • 800 patients and 385 OS events were required to provide 80% power to detect a 33% improvement in OS (HR = 0.75) at the two-sided significance level of 5% • The interim OS analysis (estimated at 50% of events for final analysis) was planned at the time of the primary independently assessed PFS analysis OS, overall survival; PFS, progression-free survival
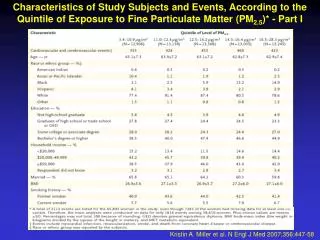
Baseline characteristics (I) ECOG PS, Eastern Cooperative Oncology Group performance status
Baseline characteristics (II) ER, estrogen receptor; FISH, fluorescence in situ hybridization; IHC, immunohistochemistry; PgR, progesterone receptor
Prior therapy for breast cancer * Numbers add up to more than 100% because patients could have received more than one therapy
Primary endpoint: Independently assessed PFSMedian follow-up: 19.3 months 100 Ptz+ T + D: median 18.5 months ∆ = 6.1 months Pla+ T + D: median 12.4 months 90 80 70 60 Progression-free survival (%) 50 40 HR = 0.6295% CI 0.51‒0.75p<0.0001 30 20 10 0 0 5 10 15 20 25 30 35 40 Time (months) n at risk 406 311 209 93 42 17 7 0 0 Ptz+ T + D 402 345 267 139 83 32 10 0 0 Pla+ T + D Stratified by prior treatment status and region D, docetaxel; PFS, progression-free survival; Pla, placebo; Ptz, pertuzumab; T, trastuzumab
Independently assessed PFS in pre-defined subgroups Favors pertuzumab Favors placebo n HR 95% CI 808 0.63 0.52‒0.76 All NoYes 432 0.63 0.49‒0.82376 0.61 0.46‒0.81 Prior (neo)adjuvant chemotherapy EuropeNorth AmericaSouth AmericaAsia 306 0.72 0.53‒0.97135 0.51 0.31‒0.84114 0.46 0.27‒0.78253 0.68 0.48‒0.95 Region <65 years≥65 years <75 years≥75 years 681 0.65 0.53‒0.80127 0.52 0.31‒0.86789 0.64 0.53‒0.7819 0.55 0.12‒2.54 Age group WhiteBlackAsianOther 480 0.62 0.49‒0.8030 0.64 0.23‒1.79261 0.68 0.49‒0.9537 0.39 0.13‒1.18 Race Visceral diseaseNon-visceral disease 630 0.55 0.45‒0.68178 0.96 0.61‒1.52 Disease type PositiveNegativeUnknown 388 0.72 0.55‒0.95408 0.55 0.42‒0.72 12 - - ER/PgR status IHC 3+ 721 0.60 0.49‒0.74 HER2 status 767 0.640.53‒0.78 FISH-positive 0 0.5 1 2 3 ER, estrogen receptor; IHC, immunohistochemistry; FISH, fluorescence in situ hybridization;PgR, progesterone receptor; PFS, progression-free survival Unstratified analyses
Overall survival: Pre-defined interim analysisMedian follow-up: 19.3 months, n = 165 OS events 100 90 80 70 60 Overall survival (%) 50 HR = 0.64*95% CI 0.47‒0.88p = 0.0053* 40 30 Ptz+ T + D: 69 events 20 Pla+ T + D: 96 events 10 0 0 5 10 15 20 25 30 35 40 45 Time (months) n at risk Ptz+ T + D Pla+ T + D 406 383 347 228 143 67 24 2 0 0 402 387 367 251 161 87 31 4 0 0 * The interim overall survival analysis did not cross the pre-specified O’Brien-Fleming stopping boundary (HR ≤0.603; p≤0.0012) D, docetaxel; OS, overall survival; Pla, placebo; Ptz, pertuzumab; T, trastuzumab
Independently reviewed objective responseIn patients with measurable disease at baseline * The statistical test result is deemed exploratory
Exploratory efficacy results By prior trastuzumab therapy
Independently assessed PFS by prior trastuzumab therapy in patients with (neo)adjuvant therapy PFS, progression-free survival
Withdrawals from study treatment in the safety population * Protocol violation, failure to return, or other
Cardiac tolerability LVEF, left ventricular ejection fraction; LVSD, left ventricular systolic dysfunction
Adverse events (all grades)≥25% incidence or ≥5% difference between arms
Conclusions The combination of pertuzumab with trastuzumab plus docetaxel, as compared with placebo plus trastuzumab plus docetaxel, when used as first-line treatment for HER2-positive metastatic breast cancer, significantly prolonged progression-free survival, with no increase in cardiac toxic effects.
![Glynn RJ, et al. N Engl J Med 2009 Mar 29 [Epub ahead of print]](https://cdn3.slideserve.com/6539248/slide1-dt.jpg)