Download
1 / 6
60 likes | 277 Vues
Recent statin trials: Reduction in primary outcome in patients with diabetes. HPS. Steno-2. 0. 10. 22. 20. Relative risk reduction (%). P < 0.0001. 30. 40. 53. 50. P = 0.007. 60. HPS: major coronary event, stroke, or revascularization

E N D
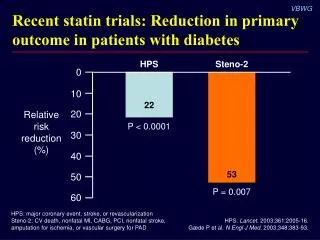
Recent statin trials: Reduction in primaryoutcome in patients with diabetes HPS Steno-2 0 10 22 20 Relativeriskreduction(%) P < 0.0001 30 40 53 50 P = 0.007 60 HPS: major coronary event, stroke, or revascularization Steno-2: CV death, nonfatal MI, CABG, PCI, nonfatal stroke,amputation for ischemia, or vascular surgery for PAD HPS. Lancet. 2003;361:2005-16. Gæde P et al. N Engl J Med. 2003;348:383-93.
CARDS: Collaborative AtoRvastatin Diabetes Study design High-risk patients with type 2 diabetes (N = 2838) Atorvastatin 10 mg Placebo Randomization completeJune 2001 Early termination June 2003 ResultsannouncedJune 2004 Plannedcompletion2005 Primary outcome: Composite of major coronary events, revascularizations, unstable angina, resuscitated cardiac arrest, and stroke Colhoun HM et al. Diabet Med. 2002;19:201-11.
CARDS: Treatment effects on lipids Total-CAverage difference 26%1.4 mmol/L (54 mg/dL) LDL-CAverage difference 40%1.2 mmol/L (46 mg/dL) 6 4 3 4 2 mmol/L 2 1 P < 0.0001 P < 0.0001 0 0 0 1 2 3 4 4.5 0 1 2 3 4 4.5 Years Years Placebo Atorvastatin Colhoun HM et al. Lancet. 2004;364:685-96.
15 Relative risk reduction 37%95% CI, 17%–52% P = 0.001 Placebo127 events 10 Cumulativehazard(%) Atorvastatin83 events 5 0 0 1 2 3 4 4.75 Years Placebo 1410 1351 1306 1022 651 305 Atorvastatin 1428 1392 1361 1074 694 328 CARDS: 37% Reduction in primary outcome Colhoun HM et al. Lancet. 2004;364:685-96.
CARDS: Consistent statin effects on components of primary outcome n (% randomized) Favorsatorvastatin Favorsplacebo Risk reduction (95% CI) Event Placebo Atorvastatin 37% (17–52)P = 0.001 Primary outcome 127 (9.0) 83 (5.8) Acute coronary events 77 (5.5) 51 (3.6) 36% (9–55) Coronaryrevascularization 34 (2.4) 24 (1.7) 31% (–16–59) Stroke 39 (2.8) 21 (1.5) 48% (11–69) 0.2 0.4 0.6 0.8 1.0 1.2 Hazard ratio Colhoun HM et al. Lancet. 2004;364:685-96.
ACP recommendations for lipid management in patients with diabetes • Lipid-lowering therapy is indicated for secondary prevention in all patients with diabetes and known coronary artery disease • Statins are indicated for primary prevention of macrovascular complications in patients with diabetes and other CV risk factors • Once statin therapy is initiated, patients should receive at least moderate doses • Routine monitoring of liver function or muscle enzymes is not recommended for patients receiving statins, except in specific circumstances Snow V et al. Ann Intern Med. 2004;140:644-9.