Download
1 / 9
100 likes | 290 Vues
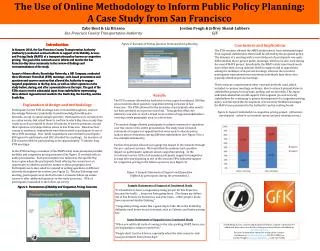
Case study – Interventions and Using the HEF to inform care planning Abasi – Referred to our team because of physical aggression towards staff at his residential home Had been arrested twice for assault and was at risk of being imprisoned. Consideration of medical disposal of case

E N D
Case study – Interventions and Using the HEF to inform care planning Abasi – • Referred to our team because of physical aggression towards staff at his residential home • Had been arrested twice for assault and was at risk of being imprisoned. Consideration of medical disposal of case • Had also been arrested multiple times for shoplifting – both planned and impulsive • Issue with hoarding in his bedroom which was spreading to the rest of the home • No ‘meaningful’ occupation’ • At risk of eviction • Difficult staff attitude towards him
What would you do? • What do you think the health inequalities are? • Which area(s) would you address first? • Which professionals would you involve?
Initial HEF • Clear focus to the work that needed to be done – • Placement at risk of breakdown • Highly restricted activity and engagement • Not registered with a GP • No recent health check carried out • No individual communication plan in place
What did we do? • Initial work – • Nursing assessment • History-taking with family and from LA and health notes • Weekly meetings with staff • Twice-weekly meetings with Abasi, arranged by him • Referred to SLT and social work • Worked with psychiatry to complete a DISCO assessment for autism • AP completed a WAIS
Interventions • Communication: • Worked with a speech and language therapist to assess communication skills and put clear guidelines for support staff in place • Used written communication for Abasi as knew he enjoyed reading and had slow verbal processing speed • Rest of our work would have been very difficult without this intervention • Started to use social stories to explain consequences of actions e.g. effect of shoplifting on shop-keeper • Outcome: • Increased engagement with staff • Participating in activities such as cooking and watching DVDs • Allowing staff to accompany him out of the home • Reduction in physical aggression – no incidences since moved placement in November 2012
Genetic and biological: • Not registered with a GP. No recent health check or health screening carried out. • Communicating with Abasi in a way that he understood and responded to meant we were able to encourage him to register with a GP and have a health screening • Psychiatrist had referred Abasi for an EEG but he had refused • Using social stories and explanations using clear words and pictures helped us encourage Abasi to attend • Outcome • Diagnosed with epilepsy in the fronto-temporal lobe. Now has an appointment at local neurology clinic to consider treatment plan • Epilepsy may be affecting his emotional regulation and impulse control – investigating whether this has bearing on the incidents of physical aggression • Now having appropriate health screening and checks
Social • Restricted activities • Used work started by OT and communication plans to discuss options for activities with Abasi • Spoke to his family about past activities and why they thought that he had stopped • Learnt about Abasi’s collections, instead of penalising him because of them • Asked staff to follow their own timetable but not to share this with Abasi. Liked novel things. • Set area in bedroom and shed and time aside for papers and magazines. Protected time to enjoy this. Staff shared in this with him • Outcome • Abasi has enrolled at college – found out that he left due to difficulties with keeping up and over-estimation of ability. SLT input arranged at new college • Still ‘collects’ things but has cleared the shed and no longer spends most of his time in there • Shares this with staff rather than hiding it
Service quality Difficulties with staff understanding Abasi’s levels of understanding and difficulties with social interaction. Difficulties with CJS (police, courts and duty solicitors) • Fedback assessment report to staff, with Abasi present. • Focussed on positives but also discussed difficulties that Abasi had • Met with manager and staff weekly to discuss how things were working • After two months decided to look for alternative placement for Abasi • Met with British Transport Police, with Abasi’s consent, to discuss his case and explain how we were working with him • Arranged a planned arrest • Attended court to explain our role • Worked with a duty solicitor and she became Abasi’s solicitor Outcome • Started again with new staff team, involved Abasi and his mum in training sessions • Living in a more ‘able’ environment • Increased interaction with staff and other people at the home • Abasi’s solicitor works with staff at the home to ensure he attends court and manages his fines • BTP put an alert on their system for a need for an appropriate adult
Behaviours • Have reduced as a consequence of the other actions • Behaviour score deals with personal behaviours – his behaviours were more to do with his social and service quality