Download
1 / 46
500 likes | 719 Vues
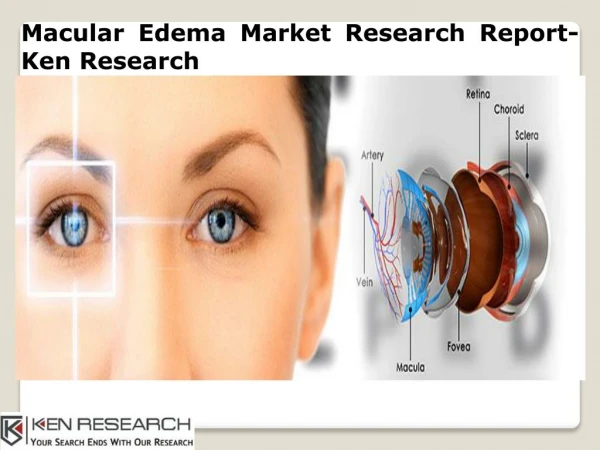
Cystoid Macular Edema A.Hekmatian MD 2010 - 1388. DEFINITION A pathological response consisting of fluid accumulation in the outer plexiform layer of the central macula that results in the formation of visible cystic spaces. KEY FEATURES

E N D
Cystoid Macular Edema A.Hekmatian MD 2010 - 1388
DEFINITION A pathological response consisting of fluid accumulation in the outer plexiform layer of the central macula that results in the formation of visible cystic spaces.
KEY FEATURES • Serous fluid accumulation in multiple cystoid spaces . • Thickening of the central macula. • Loss of the normal foveal depression. • Best detected by slit-lamp biomicroscopy with a contact or handheld lens. • A petalloid pattern of dye leakage from the perifoveal capillaries on fluorescein angiography.
ASSOCIATED FEATURES • Conjunctival injection. • Aqueous and/or vitreous cell and flare. • Optic disc edema. • A variety of ocular conditions. including aphakia, pseudophakia, inflammation. tumors, vascular abnormalities, dystrophies, medication usage, and foveal traction.
INTRODUCTION Cystoid macular edema (CME) represents a "final common pathway" response of the retina to a variety of possible insults. It has been reported in association with vascular problems (suchas diabetes and retinal vein obstruction), inflammatory conditions (such as pars planitis), inherited diseases (such as retinitis pigmentosa or dominant CME), tractional problems (such asvitreomacular traction syndrome), and use of medication suchas epinephrine (adrenaline) or latanoprost, but its most common setting is following cataract surgery.
EPIDEMIOLOGY AND PATHOGENESIS CME is a common condition associated with intraocular inflammation, vitreoretinal traction, and vascular incompetence; CME following cataract surgery is known as the Irvine-Gass syndrome.1'2 Intracapsular cataract extraction is associated with angiographically evident CME in 60% of uncomplicated cases. Extracapsular cataract extraction is associated with angiograph-ically evident CME in 20% of uncomplicated cases.
Clinically significa CME with decreased visual acuity following modern cataract surgery is seen in only 0.2 to 1.4% of eyes.
Although planned posterior capsulorrhexis at the time of phacoemulsification does not lead to an increased prevalence of CME.
Those with inadvertent rupture of the posterior capsule and/or persistent vitreous traction to anterior segment structures are at highest risk.
Neodymium:yttrium-aluminum-garnet (Nd:YAC) capsulectomy, when performed at least 3 months after cataract surgery does not appear to increase the incidence of CME.
who have any degree of retinopathy have an increasd incodence of postcataract CME.
It has been reported following retinal detachment repair and glaucoma filtering procedures as well. In phakic eyes it nearly always resolves spontaneously.
The mechanisms by which postoperative CME has been postulated to occur include vitreomacular traction, vascular compromise, and prostaglandin (PG) secretion and inflammation although the exact cause remains unknown.
Although many mechanisms may be active in the genesis of CME,the most important is intraocular inflammation.
Aside from the postcataract patient, CME occurs most commonly in the setting of diabetic retinopathy.
Panretinal photocoagulation for highrisk characteristics in diabetics can result in CME, which is usually self-limited.
Retinal vein obstructions represent another common retinal vascular cause of CME. Both branch and central vein occlusions can result in severe macular edema.
The Branch Vein Occlusion Study demonstrated a visual benefit following the application of a grid pattern of photocoagulation to the area of chronic macular edema.
The Central Retinal Vein Occlusion Study showed no visual benefit in the use of grid macular photocoagulation for the treatment of associated macular edema. However, a possible benefit may be seen in younger patients who undergo treatment.
OCULAR MANIFESTATIONS The major symptom of CME is decreased central visual acuity. Accompanying symptoms may include metamorphopsia, micropsia, scotomata, ocular irritation, photophobia, and conjunctival injection. Presenting visual acuities usually range from 20/25 (6/8) to 20/80 (6/26) but may be as poor as 20/400 .
Clinically, CME is seen best using the slit lamp and either a contact lens (e.g. Goldmann lens) or a handheld,noncontact lens (e.g., 78D, 60D) .
Individual pockets of fluid in the outer plexiform layer are seen, with the largest pockets centrally and progressively smaller cysts peripherally.
A yellow spot,believed to be due to diffusion of the luteal pigment, may be evident in the central macula. Small intraretinal and intracystic hemorrhages, microaneurysms, and telangiectasias may be seen as well .
As a result of CME, a rupture of the inner retinal cyst can occur to give a lamellar macular hole .
Prolonged CME may induce atrophy of the macular photoreceptors-visual acuity is poor, but clinical examination and fluorescein angiography may be grossly normal with the exception of a blunting of the foveal reflex .
The majority of cases occur between 4 weeks and 12 weeks after cataract surgery. Rarely, cases can occur years after surgery. Most instances of CME (approximately 75%) resolve spontaneously within 6 months .
DIAGNOISI AND ANCILLARY TESTING In eyes with dear media, clinical examination usually yields the diagnosis. Fluorescein angiography is the best ancillary test to assist in the diagnosis-in eyes with hazy media it is especially useful .
Late fluorescein angiographic pictures should be taken (up to 30 minutes following injection) to allow time for the dye to accumulate within the anatomical fovea. Also seen on fluorescein angiography is leakage from the disc and retinal vessels .
OCT provides high-resolution cross-sectional imaging of the retina analogous to B-scan ultrasonography using optical rather than acoustic reflection .
PATHOLOGY Electron microscopy shows that an intracellular accumulation of fluid produces cystoid areas and swelling of Muller's cells, a condition that is reversible. If excess fluid is present, it may break through cell membranes and accumulate extracellularly, at which stage the condition becomes irreversible.23 Histologically, large cystic spaces are seen in the outer plexiform layer.
Stepwise Approach to the Medical Management of CME FIRST STEP A topical indomethacin 1% suspension or topical ketorolac 0.5% (one drop three times a day for 2-6 weeks) may be given as prophylaxis following cataract surgery in addition to concurrent corticosteroid therapy.
SECOND STEP Corticosteroids may be beneficial in cases of persistent CME. Many patients show improvement of visual acuity within 1-2 weeks of initiation of intensive topical corticosteroid therapy." The initial treatment consists of topical prednisolone acetate I% every 2h while awake, for 3 weeks. With good clinical response, taper and discontinue over 2-3 weeks.A trial of topical therapy also allows the determination of whether the individual will respond to corticosteroid therapy with elevation of lOP. Should the pressure increase, subsequent sub- Tenon's injections should not be given. If no improvement occurs with topical therapy, posterior sub- Tenon's injection of a long-acting corticosteroid such as methylprednisolone (40mg) or triamcinolone (40mg) should be considered. A total of three injections can be given at I-month intervals. Topical and sub-Tenon's injections are used Concurrently .
Should no response or a poor response occur, systemic therapy with prednisone 40mg orally once per day for I week can be considered. Discontinue by tapering the dose over 2-3 weeks. Ranitidine 150mg should be given orally twice a day as long as the patient is receiving systemic corticosteroids. It should be noted that there is a high rate of recurrence of CME following cessation of corticosteroid therapy. Data obtained with the use of a single intravitreal injection of triamcinolone (4mg/O.1mL) also appear encouraging and may be considered for refractory cases .
THIRD STEP Favorable responses have been documented with the use of COls. Topical ketorolac four times per day for 2-3 weeks may be highly effective and can be used instead of, or in addition to, topical corticosteroids in the initial management of persistent CME . FOURTH STEP Consider oral acetazolamide 500mg/day as an adjunct to topical corticosteroids or topical CO Is in the initial management of persistent CME .