Download
1 / 47
660 likes | 1.4k Vues
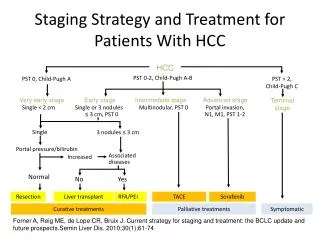
Practical Management of Cirrhotic Patients with HCC. The hepatologist’s perspective. Natural History of Hepatic Cirrhosis. Cirrhosis development. Complications development. Compensated cirrhosis. Decompensated cirrhosis. Prognosis factors. Complications risk.

E N D
Practical Management of Cirrhotic Patients with HCC The hepatologist’s perspective
Natural History of Hepatic Cirrhosis Cirrhosis development Complications development Compensated cirrhosis Decompensated cirrhosis Prognosisfactors Complicationsrisk Survival in compensated cirrhosis Survival after decompensated cirrhosis D’Amico G et al. Journal of Hepatology 2006; 44(1): 217-31
Natural History of Hepatic Cirrhosis Variceal bleeding Oesophageal varices Spontaneous bacterial peritonitis Hepaticencephalopathy Portal hypertension Ascites HCC Liver cirrhosis Hepatorenalsyndrome Hepatopulmonarysyndrome Portopulmonaryhypertension Hypermetabolism S.Fagiuoli e Gruppo di lavoro sull’Epatocarcinoma - Gestione della terapia medica dell’epatocarcinoma - Springer 2011
Practical Management of HCC Sorafenib-Treated Cirrhotic Patients • Management of the patient prior to treatment initiation • Management of the hepatopathic patient during sorafenib treatment S.Fagiuoli e Gruppo di lavoro sull’Epatocarcinoma - Gestione della terapia medica dell’epatocarcinoma - Springer 2011
Clinical Management of Patients with Chronic Hepatopathy • Management of chronic hepatopathy and treatment of its causes, in order to prevent or postpone, when possible, cirrhosis development • Management of the patient with compensated liver cirrhosis; lifestyle, antiviral treatment if indicated, follow-up and treatment of portal hypertension and its consequences • Management of decompensated cirrhosis (ascites, SBP and infections, encephalopathy, gastrointestinal bleeding, hepatorenal syndrome) S.Fagiuoli e Gruppo di lavoro sull’Epatocarcinoma - Gestione della terapia medica dell’epatocarcinoma - Springer 2011
Management of patients with HCC: the need for a multidisciplinary approach Management of HCC requires consideration of both tumour- and liver-related factors As over 85% of patients with HCC have liver cirrhosis, treatment requires input from: Hepatologist Oncologist Treatment options are diverse necessitating input from: Surgeons (transplantation and resection) Interventional radiology Hepatology Oncology PATIENT Surgery Radiology S.Fagiuoli e Gruppo di lavoro sull’Epatocarcinoma - Gestione della terapia medica dell’epatocarcinoma - Springer 2011
Summary: HCC – a complex and challenging disorder The treatment of HCC must take into account that in most patients the tumour co-exists with chronic liver disease The treatment of HCC requires a multidisciplinary approach that should include each of the following disciplines: Surgery and transplantation Interventional radiology Hepatology Oncology Peck-Radosavljevic M, et al. Eur J Gastroenterol Hepatol 2009; epub ahead of print, doi: 10.1097/MEG.0b013e328333df23.
Clinical Management of Patientswith Compensated Liver Cirrhosis
Clinical Management of Patientswith Compensated Liver Cirrhosis Cirrhosis Compensated Decompensated Basal support Monitor Liver Function (PT, Alb, Bili q 3-6 months) Varices Surveillance Antiviral treatment (HBV/HCV) HCC Surveillance (U/S, AFP q 3-6 months) Variceal Bleed Hepatorenal Syndrome SBP Ascites Encephalopathy
General Notions – 1 • Healthy lifestyle and adequate diet • Absolute abstention from toxics (alcohol, drugs, etc..) • Treatment of potential drugs dependence • Scheduling and, if necessary, adjustment of antiviral therapy • Strict clinical follow-up, both laboratory and instrumental, according to accurate diagnostic algorithms
Clinical Management of Patientswith Compensated Liver Cirrhosis Cirrhosis Compensated Decompensated Basal support Monitor Liver Function (PT, Alb, Bili q 3-6 months) Varices Surveillance Antiviral treatment (HBV/HCV) HCC Surveillance (U/S, AFP q 3-6 months) Variceal Bleed Hepatorenal Syndrome SBP Ascites Encephalopathy
Azygos vein Superior vena cava Esophagus Inferior vena cava Esophageal varices Suprahepathic vein Volume increased splein Gastric veins Portal vein pressure increases up to 20-30 mmHg Splenic vein Portal Hypertension • In a cirrhotic patient portalhypertension is related to: • Intrahepatic resistances increase • Liver structural alterations • Loss of vascular bed Portal pressure increase over 6-10 mmHg (physiological range) Gradient increase between portal and sovrahepatic pressure (HVPG) above the normal range (3-5 mmHg) Linee guida AISF 2006
Esophagoscopic view (at cardia) Azygos vein Cirrhotic liver Diaphragm Short gastric vein Esophageal branches of left gastric vein Gastroesophageal Varices – 1 • Consequences of portal hypertension • 40-90% of cirrhotic patients • 40% of Child A patients • 85% of Child C patients • >85% of HCC patients • Incidence of varices: 8%each year • Primary predictive factorof varices development:HVPG>10 mmHg AASLD Practice Guidelines. Hepatology 2007; 46(2): 608-9; Linee guida AISF 2006
Bleeding at least once in 20-40% of cirrhotic patients Bleeding incidence: 5-15% each year Primary bleeding predictive factors: varices size, red color signs, Child status Bleeding causes more than 30% of deaths 30% of cirrhotic patients die after the first bleeding episode 2/3 of patients have another bleeding episode by 1 year Esophagoscopic view (at cardia) Azygos vein Cirrhotic liver Diaphragm Short gastric vein Esophageal branches of left gastric vein Gastroesophageal Varices – 2 AASLD Practice Guidelines. Hepatology 2007; 46(2): 608-9; Linee guida AISF 2006
Prevention of a First Episode of BleedingFrom Gastroesophageal Varices Screening EGDS is recommended at diagnosis of cirrhosis Absence of varices Compensated cirrhosis: EGDS every 3 years Decompensated cirrhosis: EGDS at the time of decompensation and then every year AASLD Practice Guidelines. Hepatology 2007; 46(2): 608-9; Linee guida AISF 2006
Prevention of a First Episode of BleedingFrom Gastroesophageal Varices Small varices (<5 mm) that never bleeded Child A status and absenceof red color signs Increased risk of haemorrhage (Child B/C status or varices with red color signs) Follow-up (EGDS every year); nonselective β-blockers(no long term benefits demonstrated) Nonselective β-blockers AASLD Practice Guidelines. Hepatology 2007; 46(2): 608-9; Linee guida AISF 2006
Prevention of a First Episode of BleedingFrom Gastroesophageal Varices Medium/large varices that never bleeded NO haemorrhage risk Increased risk of haemorrhage (Child B/C status or varices with red color signs) β-blockers (endoscopic ligation or intolerance or non compliance) Nonselective β-blockersor endoscopic ligation AASLD Practice Guidelines. Hepatology 2007; 46(2): 608-9; Linee guida AISF 2006
Clinical Management of Patientswith Compensated Liver Cirrhosis Cirrhosis Compensated Decompensated Basal support Monitor Liver Function (PT, Alb, Bili q 3-6 months) Varices Surveillance Antiviral treatment (HBV/HCV) HCC Surveillance (U/S, AFP q 3-6 months) Variceal Bleed Hepatorenal Syndrome SBP Ascites Encephalopathy
HBV Cirrhosis and Antiviral Therapy • Specific antiviral therapy recommended in patientswith liver cirrhosis due to replicating B virus infection Abbreviations: ALT, alanine aminotransferase; ULN, upper limit of normal; IFN α, interferon alpha; pegIFN-α,pegylated interferon alpha; LAM, lamivudine; ADV, adefovir; ETV, entecavir; LdT, telbivudine. Lok AS et al. Hepatology 2007; 45: 507-539; Carosi G, Rizzetto M. Dig Liver Dis 2008, 40: 603-617
HBV Cirrhosis and Antiviral Therapy • Strict laboratoristic follow-up in patients with livercirrhosis due to non-replicating B virus infection Abbreviations: ALT, alanine aminotransferase; ULN, upper limit of normal; IFN α, interferon alpha; pegIFN-α,pegylated interferon alpha; LAM, lamivudine; ADV, adefovir; ETV, entecavir; LdT, telbivudine. Lok AS et al. Hepatology 2007; 45: 507-539; Carosi G, Rizzetto M. Dig Liver Dis 2008, 40: 603-617
HBV Cirrhosis and Antiviral Therapy • In specific conditions, profilaxis is also indicatedin non-replicating hepatitis B virus carriers: • In case of antitumor chemotherapy or immunosuppressant treatments (anti-TNF, anti-CD20, anti CD-56, long term steroids treatment, cyclophosphamide, methotrexate, leflunomide, cyclosporin, tacrolimus, azatioprin and micophenol acid) • Moreover, in HBsAg negative,anti HBc-positive patientswith a haematologic disease treated with fludarabin, monoclonal antibodies, marrow transplant Lok AS et al. Hepatology 2007; 45: 507-539; Carosi G, Rizzetto M. Dig Liver Dis 2008, 40: 603-617
HCV and Antiviral Therapy • Recommended in patients with compensated liver cirrhosis due to hepatitis C virus • Early liver cirrhosis • Absence of hepatic encephalopathy or ascites • Adequate hematological profile • Absence of contraindications and good compliance Ghany MG et al Hepatology 2009; 49(4): 1335-74
Which of sorafenib relatedadverse events are relevantin cirrhotic patients?
Blood and Lymphatic System Disorders Thrombocytopenia Bleeding Risk Infection Risk (SBP..) Neutropenia Lymphopenia Evaluation of Immunoprophylaxis in Hepatitis B Virus Carriers
Metabolism and Gastrointestinal Disorders Hyponatraemia Renal failure Dehydration, Ipoalbuminemia Diarrhea, vomiting Ascites
Drugs Interactions Potential enhancing of adverse events Gynaecomastia Antialdosteronic drugs
Clinical Management of Hepatopathic Patients During Sorafenib Treatment • Continue hepatopathy follow-up • Decompensation prevention • Decompensation management
Clinical Management of Patientswith Decompensated Liver Cirrhosis
Clinical Management of Patientswith Decompensated Liver Cirrhosis Cirrhosis Compensated Decompensated Variceal Bleed Hepatorenal Syndrome SBP Ascites Encephalopathy
Decompensated Cirrhosis: Triggering Events • Gastrointestinal bleeding • Infections (digestive and extradigestive) • Underlying hepatopathy flare-up • Drugs and toxics • Alcohol • Surgery • Heart failure • Dehydration • Ipertermia • Trauma • Burns • Lack of adherence or inadequate therapy … AASLD Guidelines 2005; Hepatology 2005; 41(6): 1407-32; AISF Guidelines 2005: Dig Liv Dis 2005
Cirrhosis Decompensation Variceal bleeding Oesophageal varices Spontaneous bacterial peritonitis Hepaticencephalopathy Portal hypertension Ascites Liver cirrhosis Hepatorenalsyndrome Hepatopulmonarysyndrome Portopulmonaryhypertension Hypermetabolism
Algorithm for Acute Bleeding Treatment Hematemesis and/or melena in cirrhotic patient Hemodynamic stabilization (1) Stable Unstable,prolonged bleeding Endoscopy Sengstaken Blakemore tube Not ongoing bleeding Ongoing bleeding Stable Unstable Rebleeding prevention Sclerotherapy or varices ligation Bleeding stops Bleeding continues TIPS Bleeding stops Bleeding continues Surgical shunt (1) Fluids, hemoderivates, plasma expanders, vasoactive agents (terlipressin, somatostatin, octreoide) Modificato da: Dib N et al. CMAJ 2006; 174(10): 1433-43
Secondary Bleeding Prevention β-blockers + endoscopic ligation Recurrent haemorrhages TIPS AASLD Guidelines 2007; Hepatology 2007; 46(2): 608-9; Linee guida AISF 2006
Varices bleeding refractory to medical/endoscopic therapy Prevention of rebleeding of oesophageal, gastric or ectopics (including intestinal and anorectal) varices Refractory ascites if intolerantto “large volume” paracentesis Esophagus Shunt Coronary v. Liver Stomach Spleen Portal vein Splenic vein Kidney Superior mesenteric vein Left renal vein Inferior mesenteric vein Inferior vena cava TIPS Indications Linee guida AISF 2006; AASLD Guidelines 2005: Hepatology 2005; 41(6): 1407-32
Cirrhosis Decompensation Variceal bleeding Oesophageal varices Spontaneous bacterial peritonitis Hepaticencephalopathy Portal hypertension Ascites Liver cirrhosis Hepatorenalsyndrome Hepatopulmonarysyndrome Portopulmonaryhypertension Hypermetabolism
Ascites • Non pharmacological measures: • Bed rest and sodium restriction • Fluid restriction in case of iponatriemia (<125 mEq/L) • Pharmacological measure: • Diuretic antialdosteronic drugs (spironolactone up to 400 mg/die) • In case of lack of efficacy add loop diuretics (furosemid up to 160 mg/die) Investigating SBP: broad-spectrum antibiotics if necessary AISF Guidelines 2005: Dig Liv Dis 2005; Bolondi L et al. Clin Gastroenterol Hepatol 2006; 4(11): 1395-402; Ghassemi S et al. Best Pract Res Clin Gastroenterol 2007; 21(1): 77-93
Refractory Ascites Large volume evacuative paracentesis • <5 L followed by plasmatic expansion with synthetic plasma expanders, not requiring volume expansion with albumin Larger volumes paracentesismust be followed by volume expansion preferably with albumin (8 g/L of removed ascites) TIPSif intolerance to large volume paracentesis AISF Guidelines 2005: Dig Liv Dis 2005; Bolondi L et al. Clin Gastroenterol Hepatol 2006; 4(11): 1395-402;Ghassemi S et al. Best Pract Res Clin Gastroenterol 2007; 21(1): 77-93
Varices bleeding refractory to medical/endoscopic therapy Prevention of rebleeding of oesophageal, gastric or ectopics (including intestinal and anorectal) varices Esophagus Shunt Coronary v. Liver Stomach Spleen Portal vein Splenic vein Kidney Superior mesenteric vein Left renal vein Inferior mesenteric vein Inferior vena cava TIPS Indications • Refractory ascites if intolerantto “large volume” paracentesis Linee guida AISF 2006; AASLD Guidelines 2005: Hepatology 2005; 41(6): 1407-32
Renal Failure in Cirrhotic Patients First step: differential diagnosis UNa: sodium urinary concentration; Uosm: urinary osmolarity; Posm: plasmatic osmolarity AISF Guidelines 2005: Dig Liv Dis 2005
Hepatorenal Syndrome (HRS) • Diagnosis (Ascites Club New Criteria): • Cirrhosis with ascites • Creatinin blood levels increase >1.5 mg/dl • No improvement in creatinin blood levels 2 days after diuretic treatment withdrawal and volume expansion with albumin • No recent treatment with nephrotoxic drugs • No organic renal disease (proteinuria, microematuria and ultrasound renal abnormalities) Salerno et al. GUT 2007; 56(9): 1310-1318
Hepatorenal Syndrome (HRS) Angeli P. Journal of Hepatology 2008; 48 (Suppl 1): S93-103
Hepatorenal Syndrome Management • Identify and adjust triggering causes • Volemy adjustement (diuretic treatment interruption, emoderivates, plasma-expanders) • Vasoconstrictors: • Albumin and terlipressin • Midodrin+octreoide+albumin Angeli P. Journal of Hepatology 2008; 48 (Suppl 1): S93-103
Cirrhosis Decompensation Variceal bleeding Oesophageal varices Spontaneous bacterial peritonitis Hepaticencephalopathy Portal hypertension Ascites Liver cirrhosis Hepatorenalsyndrome Hepatopulmonarysyndrome Portopulmonaryhypertension Hypermetabolism
Hepatic Encephalophaty (HE)(West-Haven) Hassanein T, et al. Am J Gastroenterol 2009; 104(6): 1392-400
Hepatic Encephalophaty (HE)Hepatic Encephalopathy Scoring Algorithm (HESA) Hassanein T, et al. Am J Gastroenterol 2009; 104(6): 1392-400
Hepatic Encephalopaty Management • Intestinal hemorrage • Uncorrect use of diuretics and/or sedative agents • Hypokaliaemia and alkalosis • Excessive protein intake • Constipation, infections • TIPS or porta-caval anastomosis • Hepatopathy worsening • Nephropathy Triggering factors adjustment Protein production and absorption • Lactulose • Lactulose • Ramified chain AA • L-ornithin L aspartate Medical therapy Als-Nielsen B et al. BMJ 2004; 1; 328(7447): 1046; AASLD Guidelines 2005: Hepatology 2005; 41(6): 1407-32
Grade III/IVHepatic Encephalopaty Management • Admission in ICU or hepatic subintensive Therapy Unit (orotracheal intubation, semi-ortopnoic position, continuous monitoring..) • Intracranic pressure monitoring • Endocranic hypertension therapy • Epileptic episodes management • Mannitol • Hypertonic saline • Hyperventilation • Steroids • Hypotermia Als-Nielsen B et al. BMJ 2004; 1; 328(7447): 1046; AASLD Guidelines 2005: Hepatology 2005; 41(6):1407-32