Vascular
Vascular. Arterial system. Aneurysmal Vascular Disease. Defined as a permanent localized enlargement of an artery to more than 1.5 times its expected diameter .

Vascular
E N D
Presentation Transcript
Vascular Arterial system
Aneurysmal Vascular Disease • Defined as a permanent localized enlargement of an artery to more than 1.5 times its expected diameter. • Aneurysms can develop at any location in the arterial tree but are most commonly found in the aorta, iliac, popliteal, and femoral arteries, in decreasing order of frequency. • The primary clinical significance of centrally located aneurysms (intrathoracic and intra-abdominal) is related to the risk of aneurysm rupture, whereas the primary clinical significance of peripheral aneurysms is related to the risk of thrombosis or embolism. • Aneurysms are classified according to anatomic site, morphology, and etiology. The most common aneurysm morphology is a fusiform, symmetrical circumferential enlargement involving all layers of the artery wall. Aneurysms may also be saccularwith aneurysmal degeneration affecting only part of the arterial circumference. • The most common etiology of aneurysms is atherosclerotic degeneration of the arterial wall. The pathogenesis is a multifactorial process involving genetic predisposition, aging, atherosclerosis, inflammation, and localized proteolytic enzyme activation. Most aneurysms occur in elderly people, and the prevalence of aneurysms increases with increasing age. Aneurysms can also occur in younger, genetically susceptible individuals with Ehlers- Danlos and Marfansyndromes. Other etiologies include localized infection that results in mycotic aneurysms and the rare tertiary stage of syphilis. Aortic aneurysms may also occur with aortic dissection. Aneurysmal enlargement can also result from hemodynamic causes such as poststenoticarterial dilation or arteriovenous fistulas. • Pseudoaneurysms(false aneurysms) are localized arterial disruptions caused by blunt or penetrating trauma, vascular intervention, or anastomotic disruption.
Incidence • The average age of patients with abdominal aortic aneurysms is 75 years, about 10 years older than the average age of patients with clinically significant arterial occlusive disease. Abdominal aortic aneurysms are more common in men than in women. • White men have a higher prevalence than black men or women. • Smoking is the most important risk factor .Prevalence of aneurysms is approximately 10% in men with hypertension or with clinical evidence of peripheral, carotid, or coronary arterial disease. There is a definite, familial incidence .
Abdominal Aortic Aneurysms(AAA) The natural history of abdominal aortic aneurysms is to enlarge and rupture. • Treatment strategies are designed to prevent this complication. • Higher enlargement rates have been associated with arterial hypertension, chronic obstructive lung disease, family history. • In less than 5% of abdominal aneurysms, the first clinical manifestation is embolization to the lower extremity. This complication is not related to the size of the aneurysm and constitutes an independent indication for repair. Risk of Rupture • The single most important factor associated with rupture is maximal cross-sectional aneurysm diameter. • AAA more than 5 .5cm should be treated even a symptomatic . • The most powerful factors that increase the risk of rupture are chronic obstructive pulmonary disease and pain.
Clinical Presentation of AAA • Most abdominal aortic aneurysms are asymptomatic before rupture,most aneurysms are discovered on routine physical examination with the palpation of a pulsatile abdominal mass or on imaging while investigating an unrelated problem. Approximately 80% of aneurysms are identified incidentally on abdominal ultrasound, computed tomography (CT), magnetic resonance imaging (MRI), or plain abdominal radiograph. • Symptomatic : Aneurysms can be associated with vague abdominal and back discomfort. Occasionally, spinal erosion is the cause of back pain, and large aneurysms may be associated with early satiety and occasionally vomiting. • Acutely expanding aneurysms produce severe, deep back pain or abdominal pain radiating to the back. This may be accompanied by tenderness to palpation of the aneurysm. This presentation often precedes rupture and urgent treatment is required. • Less than 5% of patients with abdominal aortic aneurysm have evidence of embolization, usually small, to the distal arteries of the lower extremities. As many as 12% of aneurysms present for the first time with acute aneurysm rupture. • About 5% of aneurysms present with nonspecific, idiopathic retroperitoneal fibrosis. These aneurysms are referred to as inflammatory aneurysms. They are often associated with pain, fever, and fibrosis, which may involve the uretersand cause ureteral obstruction.
Diagnosis • Physical examination is useful for the diagnosis of abdominal aortic aneurysms, especially in thin patients and patients with large aneurysms. An important feature on physical examination is detection of expansile pulsation, where the gap between both hands placed on either side of the aneurysmv widens with each systole. This finding separates the aneurysm from normal aortic pulsations, which can be normally palpated in thin subjects, particularly those with lordotic spines, and young women, and whenever a mass overlies the aorta and transmits them. • Abdominal aortic aneurysms are occasionally discovered on plain abdominal or on a lumbar spine radiograph by the characteristic “eggshell” pattern of calcification. • Abdominal ultrasound is the most widely used noninvasive test for diagnosing and following up abdominal aortic aneurysms. Ultrasound is accurate in demonstrating the presence of an aortic aneurysm and in measuring transverse diameter .Useful for screening and for surveillance of small aneurysms and may prove useful for follow-up after endovascular repair. • CT is the most precise test for imaging aortic aneurysms. CT scanning clearly demonstrates the size and extent of aortic aneurysms and their relation to renal and iliac arteries. Renal artery stenoses, accessory renal arteries, and renal and renal vein anomalies are clearly evident. CT has largely replaced arteriography for evaluation of aortic aneurysmal disease. • MRI and MR angiography accurately demonstrates aortoiliacaneurysmal disease and is useful for planning and for follow-up of endovascular repair. It is less sensitive than CT scanning in identifying accessory renal arteries and grading renal artery stenoses. • Arteriography ?
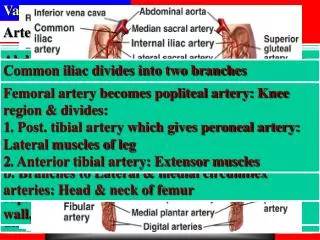
A, Ultrasonography demonstrates an abdominal aortic aneurysm. Note the posterior mural thrombus within the aneurysm sac. B, Three-dimensional CT image illustrates the presence of an infrarenal abdominal aortic aneurysm.
Treatment and Preoperative Evaluation • All patients with symptomatic AAA , and a symptomatic AAA with diameter more than 5.5 cm should be treated on elective base . • Patients with aneurysms are most often elderly and frequently have coexisting cardiac, pulmonary, or renal disease, which increases the risk of aneurysm repair. Complete preoperative evaluation and careful patient selection can reduce perioperative risk. Because history, physical examination, and electrocardiography (ECG) has been largely superseded by stress or thallium cardiac scintillation scan and the dobutamine echocardiogram. Other tests include measurement of the ejection fraction by echocardiogram or multigated acquisition scan and continuous portable ECG monitoring. Patients who are found to have significant coronary artery disease may be referred for catheter-based or surgical coronary revascularization before surgical repair of the aneurysm. • Pulmonary function studies can serve as a rough prognostic guide and should be optimized before surgical intervention. • Preoperative renal function is an important determinant of perioperative morbidity and influences the use of contrast agents in diagnostic tests or at the time of endovascular repair.
Endovascular abdominal aortic aneurysm repair involves aneurysm exclusion with an endoluminal aortic stent-graft introduced remotely, usually through the femoralartery.
RUPTURED ABDOMINAL AORTIC ANEURYSM • The most dreaded complication of abdominal aortic aneurysms is aneurysm rupture. Aneurysms can rupture freely into the peritoneal cavity or into the retroperitoneum (leaking ). Free intraperitoneal rupture is usually an anterior rupture and is usually accompanied by immediate hemodynamic collapse and a very high mortality rate. Retroperitoneal ruptures are usually posterior and may be contained by the psoas muscle and adjacent periaortic and perivertebral tissue. • Both types of rupture present with acute excruciating back and abdominal pain, accompanied by pallor, diaphoresis, syncope, and other symptoms and signs related to blood loss and hypovolemic shock. Occasionally, patients may have chest pain induced by retroperitoneal blood loss or hypovolemia, misleading the physician to suspect primary myocardial ischemia. • Patients with ruptured aortic aneurysms require immediate surgical repair. Blood should be rabidly prepared. • Resuscitation ? • Stable patients with a questionable diagnosis may undergo CT scanning. In patients not stable enough to undergo CT scanning, the presence of an aneurysm can be confirmed by bedside ultrasound. • Acutely expanding aneurysms may present with abdominal pain and tenderness on palpation. These are prone to rupture and should be repaired on an emergent basis.
Peripheral Arterial Occlusive Disease • Adverse events are due to the effects of impaired circulation on critical end organs (e.g., brain, heart, abdominal viscera) or extremities. • Atherosclerosis is the most common and is a complex, chronic inflammatory process that affects the elastic and muscular arteries. • Other causes of arterial occlusive disease, although far less common than atherosclerosis , must also be considered, especially in patients who do not fit the risk factor profile outlined. These include thromboangiitisobliterans (Buerger’sdisease), Takayasu’sarteritis, giant cell/temporal arteritis, and other less common vasculitides. • Each of these disorders has unique clinical, radiographic, and anatomic features
AtherosclerosisRisk Factors and Pathology Firmly Established Relative Factors Hypercholesterolemia Advanced age Cigarette smoking Male gender Hypertension Hypertriglyceridemia Diabetes mellitus Sedentary lifestyle Family history • The disease is both systemic and segmental,with clear predilections for certain locations within the arterial tree and relative sparing of others. The earliest lesions (i.e., fatty streaks) may be detected in childhood in susceptible individuals. • The pathologic hallmark of atherosclerosis is the atherosclerotic plaque. There are several major components of plaque: smooth muscle cells, connective tissue (matrix), lipid, and inflammatory cells (predominantly macrophages). Platelets may adhere to dysfunctional endothelium, exposed matrix, and monocytes/macrophages
Presentation of CHRONIC OCCLUSIVE DISEASE OF THE LOWER EXTREMITIES • Reproducible ischemic muscle pain resulting from inadequate oxygen delivery during exercise. Claudicationdistance is an indicator for the severity and the site is related tom the site of arterial occlusion. Eg : Symptoms or signs of occlusive disease of the bifurcation of the abdominal aorta (Leriche syndrome) include Claudication of the buttocks and thighs associated with impotence , absent pulse in both femoral arteries • As opposed to the patient with claudication, who has cramping pain with exercise, the patient with more advanced critical ischemia complains of pain at rest. • Rest pain occurs when blood flow is inadequate to meet resting metabolic requirements. In the lower extremity, ischemic rest pain is localized to the forefoot .The patient with rest pain is often awakened by severe discomfort in the forefoot and hangs the affected extremity off the bed for temporary relief of symptoms. • Patients often have trophic changes, such as muscle wasting, thinning of skin, thickening of nails, and hair loss in the distal affected limb. • Rest pain is an ominous symptom and usually requires revascularization because this form of advanced ischemia generally progresses to tissue loss. • The patient with critical ischemia is at risk for tissue infection or gangrene resulting from arterial insufficiency.
Diagnostic Modalities in Peripheral Arterial Occlusive Disease • A key principle in the treatment of peripheral atherosclerosis is the hemodynamic assessment of circulatory impairment, which assumes paramount importance in comparison to the anatomic presence or distribution of lesions. • Segmental pressure measurements in the limb can be used to localize and grade hemodynamically significant lesions, as well as the overall degree of circulatory impairment. The single most useful index is the ankle pressure, which can be obtained simply at the bedside with a handheld Doppler probe and pressure cuff. • Because the ankle pressure varies with central aortic pressure, it is commonly indexed to the brachial artery pressure as a ratio (ankle-brachial index [ABI]). In normal resting subjects, the ABI is slightly greater than unity (1.0 to 1.2). • There is a correlation between the severity of signs and symptoms of arterial insufficiency and the ABI, such that claudicants usually fall in the 0.5 to 0.7 range, whereas critical ischemia (rest pain or tissue necrosis) most commonly is associated with an ABI less than 0.4. In addition to preoperative assessment, the ABI can be used to follow up patients after arterial reconstruction as a measure of technical success or subsequent graft failure. • Exercise (treadmill) testing may be used in patients with claudication. It is particularly useful in the evaluation of patients with atypical symptoms, normal resting pulse .A normal exercise test rules out arterial insufficiency explicitly. In addition, exercise testing has been used to quantify the degree of impairment in arterial claudication; self reporting of walking distance is notoriously unreliable. • Doppler and Duplex Ultrasonography • Arteriography( preoperative ) • Computed tomography (CT) with intravenous contrast medium administration can also delineate vascular anatomy. • Magnetic resonance angiography (MRA)
Color Duplex ultrasound images with Doppler velocity profiles
Complications of Contrast Arteriography • Puncture Site or Catheter Related • Hemorrhage/hematoma • Pseudoaneurysm • Arteriovenous fistula • Atheroembolization • Local thrombosis • Contrast Agent Related • Major (anaphylactoid) sensitivity reaction • Minor sensitivity reactions • Vasodilation/hypotension • Nephrotoxicity • Hypervolemia (osmotic load)
Therapeutic Interventions in Arterial Occlusive Disease • Medical Management: Targeted to reduce progression, induce regression, and prevent morbid endpoints of lesion formation. • For all patients and the only treatment for milled claudication Risk factor management is the primary approach. • Lipid-lowering therapy uses both dietary treatment and an increasing pharmacopeia with specific effects on different lipid subclasses. These drugs include niacin, bile acid-binding resins, clofibrate, and gemfibrozil. • Smoking cessation is clearly of paramount importance. • Others :Hypertension , Diabetes mellitus, anemia, respiratory disease Antiplatelet therapy Aspirin remains the cornerstone of platelet therapy. Newer antiplatelet agents have been developed with everincreasing potency and more specific antiaggregative effects. For the present, low-dose aspirin is the most widely accepted antiplatelet prophylaxis for patients with cardiovascular disease.
Surgery • Indication 1- critically eschimic limp( what )
Surgery • Surgical Bypass Grafting • Natural vs. synthetic
In situ method of infrainguinal reconstruction. Saphenofemoral
Endovascular Surgery.Percutaneous Angioplasty, Stenting. A hemostatic arterial sheath showing the inner dilator and hemostatic valve A variety of selective catheters that are used for peripheral interventions.
Intravascular stents An inflated angioplasty balloon catheter
ACUTE THROMBOEMBOLIC DISEASE • Unlike the brain, which suffers infarction after only 4 to 8 minutes of ischemia, or the myocardium, which infarcts after 17 to 20 minutes, the lower extremity may be salvaged after up to 5 to 6 hours of profound ischemia. Etiology • I)Embolism: Cardiogenic 80%(Rheumatic valvular heart disease, Prosthetic heart valves, Atrial fibrillation , Myocardial infarction , Bacterial or fungal endocarditis). Noncardiac 10%(Aneurysmal disease, Proximal artery , Paradoxical emboli) Idiopathic 10%
aortic bifurcation known as a “saddle embolus. right popliteal artery. occlusive left femoral embolu
II) Thrombosis • Acute thrombosis generally occurs in vessels affected by preexistent atherosclerosis. As such, there is generally some degree of collateral vessel development and the resultant ischemia is often less severe than with acute embolic disease. A particularly severe form of ischemia results from distal vascular thrombosis of the extremities, which may occur in the setting of sepsis or with hypercoagulable states. The most common hypercoagulable states associated with acute arterial thrombosis are antithrombin III deficiency, lupus anticoagulant (antiphospholipid antibody), and protein C deficiency. Although usually associated with venous thrombosis, activated protein C resistance caused by the spontaneous mutations of factor V Leiden may also cause arterial thrombosis. • Acute thrombosis of a previous arterial bypass graft may also lead to recurrent ischemia. The degree of ischemia depends on the location of the graft and the original indication for surgery. Early graft occlusions (within 2 months of surgery) are usually caused by technical or judgmental errors.
Presentation and Evaluation • The classic presentation of patients with acute ischemia of the extremities may be recalled by the “five Ps”: pain, pallor, pulselessness, paresthesias, and paralysis. • Pain is the most common complaint in alert patients. The sudden onset of severe ischemic pain in a previously asymptomatic patient is most suggestive of an embolic occlusion. Patients with spontaneous thrombosis often have had chronic symptoms of claudication or various degrees of pain before the acute event. • Pallor is a common : cool, waxy-appearing white extremity with no signs of cutaneous blood flow. Conversely, a partial occlusion may result in only delayed capillary refill with pallor on elevation of the extremity and rubor on dependency. • The absence of arterial pulses on examination will alert the surgeon to both the location of the arterial occlusion and the degree of ischemia. Patients with acute arterial embolism generally have normal palpable pulses above the occlusion with a complete absence below. The pulse immediately above the occlusion may be particularly prominent with a “water-hammer” quality that results from limited arterial outflow. • A handheld continuous-wave Doppler examination plays an important role in the initial evaluation of patients with acute vessel occlusion. The presence of even monophasic Doppler signals over the pedal vessels affirms distal vascular patency and at least short-term viability of the distal tissues. Conversely , a complete absence of arterial flow is most suggestive of profound ischemia and calls for immediate revascularization.
The peripheral nerve is the tissue that is most sensitive to ischemia. As such, the degree of neurologic dysfunction is a sensitive barometer of the degree of ischemia. With mild ischemia, the findings may be subjective and subtle. Earlyparesthesiasmay be characterized as a numbness of the toes or a slight decrease of sensation of the foot compared with the contralateral extremity to light touch or pinprick. • With severe ischemia, however, profound sensory loss may lead to complete anesthesia of the foot, indicative of impending tissue loss without early revascularization. • Weakness of the extremity is another important sign of neurologic ischemia of the extremity. Patients with an aortic saddle embolus may have bilateral paralysis and anesthesia from the waist down. • In patients with severe ischemia characterized by anesthesia and paralysis, it is important to distinguish reversible from irreversible ischemic changes. Patients with prolonged ischemia have palpable firmness to the extremity muscle and stiffness to the extremity indicative of muscle rigor. Reperfusion of such an extremity does not restore function and can result in severe systemic injury. Primary amputation is the safest form of management in such cases.
Management • Because evaluation of patients with acute arterial occlusion generally differs for patients who have suffered embolic versus thrombotic occlusion, it is important to make the appropriate clinical distinction. Patients with emboli tend to have risk factors (e.g., atrial fibrillation, recent myocardial infarction, prosthetic heart valve), a more sudden onset of symptoms (no prior claudication), and unilateral findings (normal contralateral extremity). • Patients with acute arterial occlusion should be anticoagulated with an intravenous heparin bolus (5000 to 10,000 units) and begun on a continuous infusion at 1000 units/hr. • When the history and physical examination implicates an embolus as the source of occlusion, the subsequent evaluation should be simple and direct. Routine preoperative blood work and a chest radiograph are obtained, and a 12-lead electrocardiogram is performed. Because arterial emboli are removed by direct arterial cut down and removal of the embolus( Embolictomy), there is generally no need for preoperative arteriography. When the diagnosis of embolus is questionable or the site for simple arterial cutdown and arteriotomy unclear, a preoperative arteriogram may be useful to define the anatomy and guide the revascularization procedure.
Management • Arteriograms of intraarterial emboli often demonstrate an abrupt cutoff of the artery with a rounded meniscus at the site of the embolus .Conversely, the embolus may appear as an intraluminal defect with partial flow around it. • Postoperatively, when the embolus has been removed and the limb revascularized, and the patient is stable, the evaluation should be completed by documentation of the source of the embolus. In most cases, this involves transesophageal echocardiography. • Thrombotic arterial occlusion undergo an initial arteriogram to delineate the arterial anatomy and define the best mode of revascularization. In most cases, the site of thrombotic occlusion is well delineated. In patients with a satisfactory inflow and outflow vessel with a long segment of occluded vessel, the best option is generally to proceed to surgery and perform a surgical bypass procedure.
Thrombolytic Therapy: • Fibrinolytic drugs enhance conversion of plasminogen to plasmin, which is then capable of degrading fibrin clot. These agents have been used in both systemic and local fashion to achieve lysis of both arterial and venous thrombi. It is used as an important adjunct to PTA or surgical interventions that directly address the underlying atherosclerotic lesions, restoring perfusion to the downstream bed. The two major drugs in current use are urokinase and tissue plasminogen activator (tPA). Contraindications to Thrombolytic Therapy • Absolute: 1-Recent major bleeding 2-Recent stroke 3-Recent major surgery or trauma 4-Irreversible ischemia of end organ 5-Intracranial pathology 6- Recent ophthalmologic procedure • Relative: 1-History of gastrointestinal bleeding or active peptic ulcer disease 2-Underlying coagulation abnormalities 3- Uncontrolled hypertension 4-Pregnancy 5-Hemorrhagic retinopathy An important consideration in evaluating patients for thrombolytic therapy is the severity of ischemia and the time interval for restoring perfusion before irreversible tissue injury has occurred. Patients with signs of irreversibility such as major neurologic impairment should not undergo attempted thrombolysis.
Vascular Trauma • Penetrating trauma typically results in varying degrees of laceration or transection of the vessel. The severed ends of a completely transected artery often retract and undergo spasm with subsequent thrombosis. Therefore, a lacerated or incompletely transected vessel typicall bleeds more profusely than a completely transected one. • Blunt trauma results in disruption of the arterial wall, ranging in severity from small intimal flaps to extensive transmural damage with either extravasation or thrombosis. Deceleration injury causes deformation of the arterial wall. Tight plaster ,fracture . • Bleeding from a lacerated vessel can be free or contained, the latter leading to pseudoaneurysmformation. • An arteriovenous fistula is the result of a traumatic communication between an injured artery and vein. • Limb loss is more likely to result from blunt trauma and high-velocity gunshot injuries, mainly because of the significantly greater damage to bone and soft tissue of the injured extremity. Low-velocity gunshot injuries and stab wounds rarely lead to limb loss. • Iatrogenic injury may occur either at the target site of the intervention (e.g., a coronary artery) or at the access site (e.g., the common femoral artery). The latter is more common and sometimes requires surgical repair .Every cardiac catheterization or arterial line insertion is, in fact, a form of vascular injury, where the physician relies on the patient’s hemostatic mechanism to plug the hole and repair the damage..
Buerger’s disease • Buerger’s disease is exclusively associated with cigarette smoking. The disease is more prevalent in the Middle East and Asia. Occlusive lesions are predominantly seen in the muscular arteries, with a predilection for the tibial vessels. Rest pain, gangrene, and ulceration are the typical presentations. • Recurrent superficial thrombophlebitis (“phlebitis migrans”) is a characteristic feature. • The diagnosis is suspected in younger patients who are heavy smokers and do not have other atherosclerotic risk factors. • Angiography often reveals diffuse occlusion of the distal extremity vessels. The arterial involvement appears to progress in a distal to proximal fashion. • Revascularization options are therefore usually limited. The disease virtually always shows clinical remission if smoking cessation can be achieved. Sympathectomy has a limited role in patients with ulcerations.
Raynaud’s phenomenon • Raynaud’s phenomenon is characterized by recurrent, episodic vasospasm of the digits brought on by cold exposure or emotional stress. Exposure to cold initially produces pallor of the digits, followed by cyanosis, and is accompanied by pain and paresthesias. Rewarming leads to marked rubor caused by a hyperemic response. The clinical spectrum of severity is broad and may include ulceration or loss of digits in patients with protracted periods of ischemia. Progression to tissue loss implies persistent vascular occlusions beyond the vasospastic component. • Primary (Raynaud’s disease) and secondary causes are recognized. Secondary Raynaud’s phenomenon has been associated with a variety of rheumatologic, hematologic, and traumatic disorders, as well as a number of drugs and toxins. Treatment is centered around minimizing exposure to the triggering stimulus and pharmacologic (calcium channel blockers, sympatholytics) therapy. Sympathectomy may play a role in patients with severe digital ischemia and ulceration.
Others • Takayasu’s arteritis (“pulseless disease”) commonly afflicts younger female patients and has a higher prevalence in those of Eastern European or Asian descent. The arterial pathology is focused on the aorta and its major branches. Surgical treatment is often indicated for ischemic manifestations and should only be undertaken when active inflammation is under control (i.e.,normalized erythrocyte sedimentation rate). • Temporal arteritis (sometimes referred to as giant cell arteritis) predominantly afflicts patients older than 50 years of age, with a slight (2:1) female preponderance. The superficial temporal, vertebral, and major aortic arch branches may be involved. As in Takayasu’s disease, there are often signs of systemic inflammation. Ischemic symptoms are common, including claudication of facial or extremity muscles and retinal ischemia. Headache is a common symptom. Blindness, usually irreversible, is a dreaded complication. Once the clinical diagnosis is suspected, treatment must be prompt and consists of high-dose corticosteroid therapy. Surgery is rarely indicated except in cases of major aortic branch involvement with ischemic symptoms.
Aortic dissection • Acute aortic dissection is the most common catastrophic event involving the aorta. A tear in the intima allows blood to escape from the true lumen of the aorta, dissects the aortic layers, and reroutes some of the blood through a newly formed false channel. The weakened aortic wall is highly susceptible to acute rupture and chronically prone to progressive dilation. Arterial hypertension and connective tissue disorders (particularly Marfan syndrome) may predispose patients to dissection. The cause of the initial tear remains unknown, but the histology of the aortic wall typically exhibits medial degeneration.
Classification Left, Stanford type A, DeBakey types I and II. Right, Stanford type B, DeBakey type III.
Conventionally, aortic dissection is termed acute when a clinical diagnosis is made within 14 days following the onset of symptoms and chronic after 14 days. • When a dissection involves the ascending aorta, it is commonly referred to as a Stanford type A. • Dissection without involvement of the ascending aorta—most often with the intimal tear in the descending thoracic aorta—is referred to as a Stanford type B or DeBakey type III. • DeBakey classification further distinguishes ascending aortic dissection with involvement of the descending thoracic aorta (DeBakey type I) from ascending aortic dissection without involvement of the descending thoracic aorta (DeBakey type II). • Approximately 20% of aortic aneurysms and dissections are related to hereditary connective tissue disorders.Marfan syndrome is the most common of these disorders. Skeletal, ocular, and cardiovascular complications characterize Marfan syndrome, with aortic aneurysm and dissection as the major cause of morbidity and mortality.
AORTIC DISSECTIONClinical Presentation • Abrupt excruciating pain epitomizes the onset of acute aortic dissection. Chest pain is present in about two thirds of patients and back pain invariably accompanies dissections that begin distal to the aortic arch. Pain may migrate as the dissection progresses distally. Patients with ascending aortic dissections may have associated aortic valve insufficiency with dyspnea and a diagnostic loud pansystolic murmur. • Other acute symptoms and signs related to aortic branch occlusion can cause cerebral infarction, myocardial infarction, abdominal malperfusion, limb ischemia, and paraplegia. • Serious life-threatening complications typically occur during the acute phase, and surgery on the acutely dissected aorta is high risk, associated with considerable bleeding due to the friability of the aortic wall.
Treatment • Acute type A dissection most often requires emergency surgical repair because of the associated high risk of death due to rupture, tamponade, and/or aortic valve insufficiency .The patient who is unstable with suspected type A acute aortic dissection is immediately transferred to the operating room and evaluated by TEE. If dissection is confirmed then repair is undertaken at once . Surgery in the case of the hemodynamically stable patient is less urgent, and the patient is first transferred to an acute care setting until confirmation of the diagnosis is made. • For acute type B aortic dissection the treatment of choice is generally medical therapy aimed at pain control and the correction of hypertension . Patients are admitted to an intensive care unit and observed closely. Surgical repair is most often reserved for dissection complicated by aortic rupture, abdominal malperfusion, limb ischemia, intractable pain, or uncontrollable hypertension. Approximately 20% of patients . with acute type B aortic dissection require surgical therapy
Arteriovenous Fistula • Abnormal connection between artery and vein, congenital or acquired, located anywhere in body • • Congenital: systemic effect is minimal; usually noted in infancy or childhood • • Acquired: enlarges rapidly, can cause heart failure; continuous bruit be heard; palpable thrill and increased skin temperature; proximal vein dilatation, diminished distal pulse, distal coolness • • Magnetic resonance imaging (MRI) is study of choice for peripheral arteriovenous malformation; angiography precisely delineates arteriovenous fistula • Treatment • • Monitor small peripheral fistulas • • If treatment is needed, most are managed with radiographic embolization: head and neck, pelvis best • • Operative management: ligate all feeding vessels
Carotid Body Tumor • Carotid body: normally 3–6 mm; nest of chemoreceptor cells of neuroectodermal origin; responds to decrease in PO2, increase in PCO2, decrease in pH, or increase in blood temperature • • Tumors of carotid body: cervical chemodectomas, 10% metastatic; • Symptoms and signs include slow enlargement of asymptomatic cervical mass; rarely, hypertension secondary to release of catecholamines; rarely, cranial nerve dysfunction from tumor extension; mass mobile in horizontal plane but not vertical plane • • Duplex ultrasound is often diagnostic • Differential Diagnosis • • Metastatic nodes from squamous cell cancer • • Thyroid cancer • • Carotid aneurysm • Treatment • • Preferred treatment is complete excision and arterial reconstruction if possible • • Complications: >50% incidence of cranial nerve dysfunction after resection