Comprehensive Diabetes Management: Patient Review and Examination Techniques
This document outlines a structured approach for conducting a comprehensive review and examination of diabetic patients. It includes detailed histories, assessing diabetes control, complications, and lifestyle factors. Key components of the examination process include opthalmoscopy for diabetic retinopathy, cardiovascular assessments, and peripheral neurological evaluations. The objective is to enhance patient care by identifying risk factors, complications, and management strategies relevant to diabetes management, thereby enabling targeted interventions to improve outcomes.

Comprehensive Diabetes Management: Patient Review and Examination Techniques
E N D
Presentation Transcript
Diabetic Station ISCEs
ISCE’s 2011 Ask Dr. Clarke says: • T2DM (diagnosed 5 weeks ago) with previous stroke • Retinal changes and peripheral neuropathy • People did lots of different things: • Opthalmoscopy • Peripheral neuro/arterial/venous examination • BP • Full Neuro • Questions • Definitions of diabetes/IGT • Dietary advice • Foot care
Objectives • History for diabetic patients • Examination for diabetic patients • List of things to learn about for the station
Section 1 History
Station 1 • Bertie Hancock – 53 years old – Office Manager in a local building society • Insulin-dependent diabetic “Perform a diabetic review”
The History Diabetic Station
Process Diabetic Control Complications Remaining History
History Diabetic Control • How, why and when diagnosed? • How is your diabetic control? Which type are you? • What are your normal blood sugars? • HbA1c? • Hypos – do you get symptoms? • Hypers – (implications for changing regime) when do you get these? • What do you control your diabetes with (diet, medications, insulin) • If on insulin – how long? Any problems injecting? • Who else is involved in care - where, by whom? • Last review and outcome • Best and worst health (acute deterioration and exacerbations, admissions to hospital/ITU)
History Complications • Hospital admissions? For what? ITU? • Visual disturbances? (If so, results of last review) • Syncope? Postural hypotension? • Strokes or TIAs? • Heart disease? Chest pain? • Renal disease? (If so, results of last review) • Claudication? Peripheral Vascular disease (PVD)? • Erectile dysfunction? • Ulcers? Gait problems? TIA’s, Strokes? Eyes? MI’s? Gastroparesis? Kidneys? Penis? Leg ulcers? Peripheral neuropathy?
History Remaining History • Cardiovascular risk factors • Smoking • Alcohol • Cholesterol • Blood pressure • Diet • Sleep quality • Weight (and height) • Employment, housing, social support • Stress • Drugs and allergies • Sexual relationships • Depression screen • Family history of DM
Section 2 Examination
Patient • Eddie Bloomer is a 63-year old retired postman who has been a type-2 diabetic for 20 years. “Perform a diabetic review”
Examination Diabetes Station
Examination Suggestion ONLY: “Which aspect of your diabetes or it’s complications/symptoms affects your life the most/are you most worried about?” • Ophthalmoscopy • Cardiovascular examination • Neurological assessment • Diabetic foot
(Brief) Peripheral Examination • Marks from insulin • Dupytren’s Contracture • Carpel Tunnel (look for surgical scars) • Measure BP
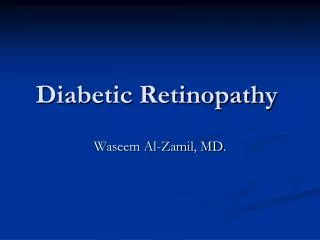
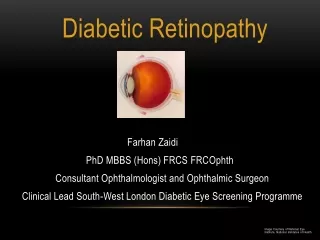
Diabetic retinopathy • Eyes of patient may already be dilated (tropicamide) • Test visual acuity (Snellen Charts) + fundoscopy • Occurs due to vascular permeability and vascular occlusion (microvascular) • Types: • Background retinopathy • Diabetic maculopathy • Pre-proliferative retinopathy • Proliferative retinopathy • Microaneurysms > dot and blot haemorrhages > hard exudates > retinal oedema > flame haemorrhages > cotton wool spots > neovascularisation • Investigation: GOLD standard: Retinal photography (Digital Retinal Imaging) • Management: MDT, NICE referral criteria (?photocoagulation/vitrectomy/Intravitreal anti-VEGF), good diabetic control,.
Opthalmoscopy • Wash handsIntroduce yourself to patient • Ask permission to examine patient's eyes • Reposition the patient sitting down in a chair opposite you • Explain that you will be using a bright light and getting very close - reassure them that they can breath normally and stop you if they feel uncomfortable. • Use the ophthalmoscope in a dimly lit room • Ophthalmoscopy is much more effective when the patient has dilated pupils - do this with Tropicamide eye drops, but warn the patient that their vision will be blurry for a few hours and that they can't drive until this has worn off. Drops should be applied about 10minutes before you begin the examination • Check that the ophthalmoscope turns on properly, turn onto biggest light and set focussing wheel to zero (you can adjust the focus later when you are looking at the patient's retina) • Ask the patient them to look at a distant object • Stand/kneel/sit in front of the patients (which ever is comfortable) • Use the ophthalmoscope with the same eye as the eye that you're examining in the patient (e.g. if you're looking at their left eye - look through the ophthalmoscope using your left eye), and use the hand of the same side to hold the ophthalmoscope • At about an arms length, just off centre (so that the patient is looking just over your ear), shine the light into their eyes and look through the lens for the 'red reflex' • Then, move towards the patient at the same angle, focusing in on the pupil. You should begin to see the disk (or, depending on your angle, other vessels in the eyes). Approach the patient slowly, and use your opposite hand (which is not holding the ophthalmoscope) to hold their forehead still and stop you bumping into them • Locate the optic disc (nasal side of eye) by moving the ophthalmoscope around • Assess colour, cup and contour of the disc • Then follow the four major branches of the optic vessels to look for tortuosity, haemorrhage, ischaemia and silver wiring (going superior and inferior to the disc, both nasally and temporally) • Look to the superior, inferior, nasal and temporal margins of the retina • Finally, ask the patient to briefly look into the light in order to assess the macular Thank the patientPresent your findings with the examiner - comment on: appearance of vessels, if you can see haemorrhages, cotton wool spots, assess colour of retina, look for; cherry red spot, dot, blot or flame haemorrhages, exudates etc.
Cardiovascular Examination • JVP • Feel the apex beat • Listen to the heart • Listen to the lung bases
Diabetic nephropathy • Glomerular changes (glomerulosclerosis - microvascular) • Initially microalbuminuria • Progresses to proteinuria • Activation of RAAS system (macrovascular) • Investigation: “Collect an early morning urine sample. Test the albumin:creatinine ratio” • U+Es (eGFR) • FBC (normocytic normochromic anaemia) • Full lipid profile (mixed dyslipidaemia) • Exclude other causes: MSU, ESR, ANA, Anti-GBM, Calcium, urate, plasma and urinary protein electrophoresis, Renal tract US. • Treatment: Good control of diabetes, patient eduction, start on an ACE-inhibitor (reduces proteinuria; or ARB), refer is eGFR <30
Diabetic neuropathy Painful neuropathy (Diabetic amyotrophy) • Burning sensation of lower limbs, worse at night • Examine: Ankle reflexes (↓), vibration and pressures sensation (↓), Inspect and test tone of legs (muscular weakness and wasting (late sign)); Complications - small muscles of hand, high arched feet, neuropathic ulcers, neuropathic joints • Diagnosis: Clinical (may do nerve conduction studies) • Treatment: WHO analgesic ladder > Amitrityline (or Duloextine) / anticonvulsants > Pain Specialist Autonomic neuropathy • Postural hypotension (neurones are not able to sense the natural drop in BP as person stands up and therefore does not compensate by ↑ HR so person becomes light-headed) • Examine: Lying and standing BP, (barium meal for gastroparesis) • Gastroparesis • Treatment: Patient education, avoid postural-hypotension-causing drugs, ?fludrocortisone Erectile dysfunction • Due to blood flow and neurological problems • Treatment: PDE5 inhibitors (Sildenafil/Viagra) Mononeuritis multiplex
Diabetic Foot • Pain is good – pain protects! 1. Inspection • Pick up shoes and look at soles • Colour • Deformities • Skin changes 2. Neurology • Vibration • Proprioception • Fine tough and pressure (with monofilament) • Reflexes (loss of ankle reflex) • Glove and stocking sensory neuropathy 3. Vascular assessment • Pulses • Temperature • CRT • “I would also like to test the ABPI’s if I was significantly concerned about the vascular status of these legs)” 4. Gait assessment
Section 3 Differentials, Investigations and Management Plan
Advice • Create a ‘problem list’ (i.e. painful neuropathy) and suggest investigation and management of this (i.e. MDT, WHO pain ladder, amitriptyline, exercise etc.) • Do differentials on the initial presentation of diabetes (and if it was acute, management of this) • Investigations and management may be one and the same • Screening is investigation AND management • Talk specifically about what you examined... • MDT...MDT...MDT • Specialist Diabetic Nurse, Podiatrists, GP, Endocrinologists, Orthotists, Opthalmologists, Renal Physicians
Some management things • Glycaemic control • Diet • Drugs • Sulphonylureas (hypoglycaemia and weight gain) • Biguanides (do not cause hypoglycaemia, may aid weight loss) • Insulin sensitisers (hepatotoxicity) • Insulin formulations • SC • Tailored to suit individual patients • Soluble insulin – fast-acting and short-acting, good for fine control • Prolonged acting insulin – less accuracy and slower onset than soluble • Complications of treatment • Lipoatrophy and lipohypertrophyat injection site • Weight gain • Hypoglycaemia
List of things to learn/Questions • Mechanisms of drugs • Some facts of diabetes physiology/pathology • Presentation and management of diabetic emergencies • DKA • HONK • Hypoglycaemia • SIGN Guidelines – Risk Stratification of diabetic foot • WHO Criteria for diagnosing diabetes • Diabetic ‘sick rules’ • Other special situations: surgery, adolescence, pregnancy, gestational diabetes, driving, employment.