Download
1 / 24
320 likes | 2.74k Vues
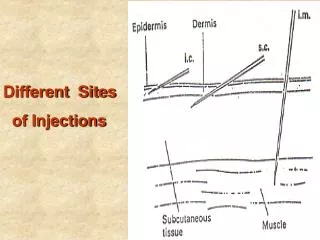
Intradermal injections & Interpretation of Mantoux Tests. Intradermal Injections. Why? Dx. Allergies ie;________________ Dx. Specific diseases ie__________ Dx. Impaired immune system. Tuberculosis. Infection caused by the aerobic bacterium, Mycobacterium tuberculosis

E N D
Intradermal Injections • Why? • Dx. Allergies ie;________________ • Dx. Specific diseases ie__________ • Dx. Impaired immune system
Tuberculosis • Infection caused by the aerobic bacterium, Mycobacteriumtuberculosis • TB kills more than 2 million people per year • Within 20 yrs-1 billion new cases of TB • 200 million will get sick • 35 million will die • More dangerous because of: • lack of health services in some parts of world • Spread of HIV/AIDS • Emergence of multi-drug resistant TB
How? Spread by droplets emitted by infected people when they are coughing, sneezing, laughing and singing • Left untreated active TB pt.s could infect 10 to 15 people each year • S & S? -cough, night sweats, chest pain, tightness, fatigue, anorexia, weight loss, low-grade fever, often persistent cough, productive with purulent yellow-green hemoptysis (bloody) sputum
Most “primary infections” are not active, but can lay dormant for years • Can invade almost any tissue in body • Most common in lungs • In lungs, small area becomes inflamed-causes immune response-some can escape & be carried to lymph • Can be necrotic @ lung site, creates cavities-can fill with infectious material • Pt. can cough up some material in sputum • Site can heal-scar tissue-(ghon) tubercule lesion
Some become active • Infectious process progresses & develops into active TB • Primary in lungs spreads • Outside lungs called Extrapulmonary TB- Infections in kidneys, bones, meninges, GI tract, lymph nodes, pericardium • Pt.s are infectious when symptoms appear
At Risk groups • In frequent contact with infected person • Immune disfunction or HIV • Living in crowded areas ie_________ • Elderly, homeless • Minorities • IV drug abusers, alcoholics • Foreign immigrants- Mexico, Philipines, Vietnam
Diagnosis (DX) • High risk exposure? • Sputum culture • Acid-fast smears of potential body flds • S & S • Chest xrays • Pneumonia that won’t heal • TB skin test
TB Skin Test • Infected pt.s immune response causes a reaction to the intradermally injected tuberculin • ***Tuberculin is a protein fraction of the tubercule bacillus**** • PROCEDURE IN LAB MANUAL • 0.1 mLs. injected under the skin • Produces wheal on skin -called raising a wheal
When to Assess A Mantoux • Mantoux test are given as a “two-step” test • 5TU’s are injected intradermally on the volar aspect of the forearm • The area is assess 48 to 72 hours later • If the first step is negative (<10mm) then the second step is administered 1-4 weeks later in the opposite arm • The area is assessed 48 to 72 hours later • The only way to diagnose active TB is with a sputum specimen
Reading the Mantoux Test • 48-72 hours (no longer) • Measuring with calipers in millimetres • Canadian guidelines • Negative – no induration (thickened local area of skin reaction, don’t measure redness) • Positive • 0-4mm- TB risk factors & immuncomp. • 5-9mm- + if pt. close contact with TB or pt. has an abnormal CXR • 10 or > 10mm. + for pt. who is healthy with no known TB risks
CDC Guidlelines (USA) • Negative – no induration (thickened local area of skin reaction, don’t measure redness) • Positive • 5mm. or > in persons with HIV infection,close contact, CXR of old, healed TB • 10mm. considered exposed/infection with high risk groups including HCW, foreign borne from hi risk areas-Asia, Africa, Latin America, medical conditions placing them at hi risk, LTC • 15 mm. is always considered positive **BCG (bacille Calmette-Guerin not TB. If greater than 10 mm., may be new infection may be + up to 9mm. as response to vaccine
Visual guide • The individual in the following slides gave permission for the pictures to be used for teaching purposes. We assured their anonymity so please do not ask details regarding the individual.
A positive Mantoux Skin Test Note the ERYTHEMA (redness) around the outside edges Note the INDURATION (red raised area) in the centre
A positive Mantoux Skin Test Note the ERYTHEMA (redness) around the outside edges Note the INDURATION (red raised area) in the centre
Measuring Devices Mantoux Measuring Devices
Measure the diameter of the induration horizontally and record the results in mm’s
This type of measuring device can but used but the caliper type shown in the previous slide is easier to use and more precise
Measure induration horizontally not vertically Measure the induration only. Do not measure the erythema. Results are recorded in mm’s not “neg” or “pos”
Contraindications • Severe blistering tuberculin reactions • Active or past hx of TB • Extensive burns or skin conditions like eczema, psoriasis, PUPPP syndrome • Major viral infections • Immunization with a live virus in the past month
Eligible for testing • Pregnant • If ill with cold • Had BCG • Recent immunization with a non-live virus vaccine • Hx. Of postive TB test
Cause of False negatives • Poor injection technique-non wheal or bleb • Immune suppressed ie: elderly, corticosteriods, cancer tx • Malnutrition • Severe illness Causes of False Positives • Had BCG • Non-tuberculous mycobacteria-uncommon
Treatment-Antituberculotics • Isoniazid • pyrazinamide(Tebrazid) • rifampin (Rofact)antit & antibiotic • ethambutol hydrochoride(Etibi)