Download
1 / 26
380 likes | 854 Vues
DR.SANDEEP SAINI LLRM COLLEGE MEERUT U.P. INDIA. ANESTHESIA FOR A PATIENT OF MITRAL STENOSIS. INDEX. INTRODUCTION ETIOLOGY & PATHOLOGY PATHOPHYSIOLOGY

E N D
DR.SANDEEP SAINI LLRM COLLEGE MEERUT U.P. INDIA ANESTHESIA FOR A PATIENT OF MITRAL STENOSIS
INDEX • INTRODUCTION • ETIOLOGY & PATHOLOGY • PATHOPHYSIOLOGY • SYMPTOMS AND SIGNS • DIAGNOSIS • ANESTHETIC MANAGEMENT
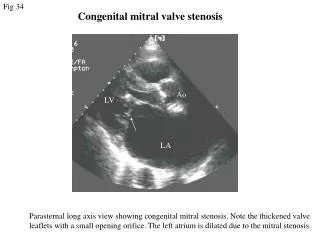
INTRODUCTION- Mitral stenosis is the narrowing of mitral orifice as a result of diffuse thickening of valve leaflets by fibrous tissue and calcific deposits. • ETIOLOGY AND PATHOLOGY-Most common cause of mitral stenosis is rheumatic heart disease. • Females are affected more than males. • Less common – carcinoid syndrome, left atrial myxoma, cor triatriatum, rheumatoid arthritis, systemic lupus erythematosus congenital. • Thickening of valve leaflets and cusps become rigid. • Fusion of mitral commissures. • Shortening and fusion of chordae tendinae. • All the changes leads to funnel shaped (fish mouth) valve. • Calcification immobilize the leaflets and narrows the orifice further.
PATHOPHYSIOLOGY • Cardiac changes- • Normal valve area: 4-6 cm2 • Mild mitral stenosis: • MVA 1.5-2.5 cm2 • Minimal symptoms • Mod mitral stenosis • MVA 1.0-1.5 cm2 usually does not produce symptoms at rest • Severe mitral stenosis • MVA < 1.0 cm2 • Symptoms at rest • Mean gradient: • >10 mmHg Severe • 5-10 mmHg Moderate • <5 mmHg Mild
Pulmonary changes • Pulmonary arterial hypertension results as- • 1)Increased left atrial pressure. • 2)Pulmonary arterial constriction. • 3)Interstitial edema in the wall of the small pulmonary vessels. • 4)Organic obliterative changes in the pulmonary vascular bed. • At last if there is severe pulmonary arterial hypertension→Tricuspid regurgitation Pulmonary in competence Rt sided heart failure
HEMODYNAMIC CHANGES THAT OCCURS AT VARIOUS STAGES OF SEVERITY OF MITRAL STENOSIS
Symptoms • Breathlessness • Fatigue • Oedema, ascites • Palpitation • Haemoptysis • Cough • Chest pain • Hoarseness • Mitral facies or malar flush • Symptoms of thromboembolic complications (e.g. stroke, ischaemic limb) • Are worsened by conditions that demand increase in cardiac output. • Exertion,fever, anemia, pregnancy, thyrotoxicosis
NYHA FUNCTIONAL CLASSIFICATION OF PATIENT WITH HEART DISEASE • CLASS Ι -Asymptomatic • CLASS ΙΙ –Symptoms with ordinary activity but comfortable at rest. • CLASS ΙΙΙ –Symptoms with minimal activity but comfortable at rest. • CLASS ΙV – Symptoms at rest
Signs Palpation: • Small volume pulse • Tapping apex-palpable S1 • Palpable S2 • Atrial fibrillation • Signs of raised pulmonary capillary pressure • Crepitations, pulmonary oedema, effusions • Signs of pulmonary hypertension • RV heave, loud P2 • Auscultation: • Loud S1 • P2 component accentuated. • A2-P2 Split. • S2 to OS interval inversely proportional to severity • Diastolic rumble: length proportional to severity • In severe MS with low flow- S1, OS & rumble may be inaudible
Lab examination • Chest x-ray • Straightening of left border of cardiac silhouette. • Prominent main pulmonary arteries. • Dilation of the upper lob pulmonary veins. • Backward displacement of the esophagus by enlarged left atria.
ELECTROCARDIOGRAPHY • The ECG may show LA enlargement, • Manifest as a P wave lasting> 0.12 msec with prominent negative deflection of its terminal component (duration: > 0.04 msec; amplitude: >0.10 mV) in V1; • Broad, notched P waves in lead II; or both. • Low voltage in V1, • Right axis QRS deviation, and tall R waves in V1 suggest RV hypertrophy
Echocardiography • Diagnosis of Mitral Stenosis • Assessment of hemodynamic severity • mean gradient, mitral valve area, pulmonary artery pressure • Assessment of right ventricular size and function. • Diagnosis and assessment of concomitant valvular lesions • Reevaluation of patients with known MS with changing symptoms or signs. • F/U of asymptomatic patients with mod-severe MS
Diagnosis • History • Symptoms • Signs on physical examination • X-ray chest • Electrocardiogram • Echocardiography
Anesthetic management • The main objectives are- To maintain sinus rhythm To avoid tachycardia To avoid large increase in cardiac output To avoid hypovolemia and fluid overload. A thorough history and examination to be done. Investigation- Hemogram Blood sugar ,blood urea ,s.creatinine x-ray chest Electrocardiogram Echocardiography
PREOPERATIVE MEDICATIONS • Antianxiety drugs decrease tachycardia associated with anxiety. • Drugs used for heart rate control should be continued until the time of surgery. • If diuretics are used treat hypovolemia and hypokalemia if associated. • For minor procedures continue the anticoagulant therapy. • For major surgery discontinue. • For regional anesthesia anticoagulant tests should be performed. • ANESTHESIA TECHNIQUE-Patients may be very sensitive to the vasodilating effect of spinal and epidural anesthesia. Epidural is preferable over spinal anesthesia because of the more gradual onset.
General Anesthesia • Premedication -Avoid premedication with anticholinergics to avoid tachycardia. opioiods like fentanyl are used to give analgesia. • Induction –Induction can be achieved with any available iv induction agent except KETAMINE as it increases heart rate and blood pressure. • For muscle relaxation agents that do not release histamine are preferred as histamine causes tachycardia and hypotension. • Steroidal group of muscle relaxants does not cause histamine release. Example are- VECURONIUM, ROCURONIUM, PANCURONIUM. • Benzylisoquinolinium group causes histamine release. Example are –ATRACURIUM, CISATRACURIUM, MIVACURIUM. • Succinylcholine also causes slight release in histamine.
Maintenance • Accomplished byuse of drugs with minimal effects on heart rate, contractility, systemic and pulmonary vascular resistance. • Achieved by –nitrous oxide & opioid. low conc. Of volatile anesthetic • For muscle relaxation vecuronium is preferred. • Avoid light anesthesia. • Intra-op fluid administration should be carefully titrated because these patients are very susceptible to volume overload and the development of pulmonary edema. • Monitoring • Noninvasive monitoring like HR, BP , ECG, RR, SpO2. • Invasive monitoring depends upon-Complexity of the operative procedure. -Magnitude of physiological impairment. • Transesophageal echocardiography could be useful in patients with symptomatic mitral stenosis undergoing major surgery.
In symptomatic patients and major surgery continuous monitoring of IBP , pulmonary artery pressure and left atrial pressure should be considered. • If there is intra-op tachycardia –deepen the plane β-blocker eg. Esmolol and propranolol. • If hypotension occurs phenylephrine is preferred over ephedrine because it lacks the β adrenergic activity. • If atrial fibrillation occurs ventricular rate is controlled with diltiazem and digoxin. • For sudden supraventricular tachycardia –cardioversion. • Reversal of anesthesia. • Reversalnondepolarising muscle relaxants is achieved slowly with neostigmine and glycopyrrolate to reduce drug induced tachycardia caused by glycopyrrolate. • Post operative management . • Proper pain managementto avoid tachycardia. • Risk of pulmonary edema and right heart failure continue so cardiovascular monitoring should be continued. • Oxygen supplementation until adequate oxygenation is established. • Management of post op hypothermia and shivering.
Thank You……….