Download

1 / 49
490 likes | 670 Vues
The New Health Care Reform: Explaining Changes To Medicare Beneficiaries. On March 23, 2010, President Obama Signed Into Law THE PATIENT PROTECTION AND AFFORDABLE CARE ACT. Followed Closely On Its Heels Was THE HEALTH CARE AND EDUCATION RECONCILATION ACT

E N D
The New Health Care Reform: Explaining Changes To Medicare Beneficiaries
On March 23, 2010, President Obama Signed Into Law THE PATIENT PROTECTION AND AFFORDABLE CARE ACT
Followed Closely On Its Heels Was THE HEALTH CARE AND EDUCATION RECONCILATION ACT Signed Into Law March 30, 2010
Taken Together These Pieces of Legislation Represent the Current Health Care Reform
After nearly two years of public debate, demonstration, and intensive lobbying, we now have the most comprehensive change in the American Health Care System since the enactment of Medicare & Medicaid in 1965.
New Legislation Contains Far Reaching Provisions Aimed At: • Reducing the number of Americans • without health coverage • Expanding eligibility for Medicaid • Reforming insurance eligibility standards • Sponsoring a system of State Based • Insurance Exchanges through which individual • consumers and small employers can gain access • to health insurance at better/reduced rates
Provisions in Effect for 2010 • Health insurers cannot eliminate existing coverage • based on discovery of a pre-existing condition • Health insurers cannot deny newcoverage to children • because of a pre-existing condition • Health insurers are required to permit dependent • children to remain on health insurance plans up to age 26 • Lifetime caps on health insurance benefits are prohibited • Requires emergency services that are out of network be • billed at in network rates
Provisions in Effect for 2014 • Private insurers will no longer be able to turn away adult individuals • with pre-existing conditions or charge higher premium rates based • on those conditions • Health Insurance Exchanges • These are state based insurance markets enabling individuals and • small businesses to purchase health insurance • Employer Mandated Health Insurance Coverage for Employees • Individual Mandated Insurance Coverage • Federally Funded Health Insurance Subsidies • Small Business Health Care Assistance
High Risk Pools temporary provisions (effective 2010) have been made to provide coverage for adults who have been excluded by insurers due to pre-existing conditions. These pools will expire in 2014 when the pre-existing condition ban goes into effect.
High Risk Pools • To qualify: • individuals must demonstrate that they: • Have been uninsured for at least 6 months • Have been denied coverage due to pre-existing • conditions • Monthly costs: • WILL be based on the costs for general health • insurance population • WILL NOT be able to vary more than 4 to 1 • Out of pocket expenses are capped at • $5,950 annually for an individual and • $11,900 annually for a family
Provisions in Effect for 2014 • Health Insurance Exchanges • State –based insurance markets based • on Massachusetts “Health Connector System” • Transparency in benefits and pricing for • individuals and small businesses • At least one guaranteed low cost selection • option
Provisions in Effect for 2014 • Employer Mandate • Business with 50 employees or more will be required • to provide insurance coverage or face a $2,000 • penalty per employee not covered • Individual Mandate • Most Americans will be required to have insurance • coverage or face fines • $95 annually for 2014 • $695 or 25% of (?) whichever is less by 2016 • Low income individuals are exempt if lowest insurance • plan cost exceeds 8% of individual’s income – these • individuals will likely be eligible for Medicaid
Provisions in Effect for 2014 • Health Insurance Subsidies • Subsidies will be available to help individuals and • families afford the mandatory insurance premiums • Subsidies will be on a graduated scale – lower incomes • receiving larger subsidies • Example – family of 4 with a total income of $88,000 • or less will be eligible for subsidies
Provisions in Effect for 2014 Small Business Health Care Assistance States will be required to set up Small Business Health Plan Option Programs (SHOP) in which small business will be able to pool together to buy insurance Small business are defined as no more than 100 employees – however states can limit SHOP to employers with 50 employees or less Effective 2010 – Small business are provided with federal tax credit until SHOP is implemented in 2014
Provisions in Effect for 2014 • Nursing Home/Long Term Care Facilities • Transparency & Improvement Program • Expanding existing requirements for • Nursing/LTC facilities to provide information • to the state government on their operations: • Staff levels • Operation schedules • Wages • Organization structure • Ownership disclosure
Provisions in Effect for 2014 • Nursing Home/Long Term Care Facilities • Transparency & Improvement Program • Nursing/LTC facilities must include dementia management program following federal guidelines • Nursing/LTC facilities must provide dementia care and abuse prevention training for all existing employees and new hires • Establishes extended guidelines for national background checks for employees of Nursing/LTC facilities that have direct patient access • Nursing/LTC facilities will be required to report incidents of patient abuse
Provisions in Effect for 2014 CLASS Program provides a public, voluntary, long term program that working individuals can purchase. The program would cover home care, respite care, home modifications, transportation, and assistive technologies.
Provisions in Effect for 2014 • CLASS Program • Buy-in program funded entirely by participants • who make voluntary salary withholding from • their gross wages • Participants are entitled to guaranteed benefit • payouts of at least $50 per day for the cost of • LTC
The New Health Care Reform Impacts Medicare in a Number of Ways:
Some Provisions are directed at HEALTH CARE PROVIDERS: how Reimbursements and Subsidies are Determined and Dispersed
Some Provisions affect MEDICARE BENEFICIARIES and the Benefit Services they receive under Medicare
Some Provisions fall within the area of Improving the Quality and Performance of the Health Care System
Changes Effective In 2010 • Nursing Home Compare Medicare Website • Links to state nursing home survey and certification programs, model complaint forms, summary of complaints and information on criminal violations
Changes Effective In 2010 • Hospital Payment Rates • Reduces payments to inpatient acute care hospitals, LTC hospitals, psychiatric hospitals and rehabilitation hospitals • Therapy Cap Exceptions • Extends the process for allowing exceptions to the payment caps for physical speech and occupational therapy until 12/31/2010. Providers must submit claims for an exception.
Changes Effective In 2010 • Medicare Part B Premiums • Freezes the income threshold for beneficiaries who pay a higher Part B premium. Will be frozen at the 2010 income levels through 2019 • Special Needs Plans (SNP) • Extends the SNP program until 2014. • CMS will apply “frailty payment adjustments” • for dual SNP beneficiaries
Changes Effective In 2010 • Closing the Part D Prescription Drug • Coverage Gap (the Donut Hole) • For 2010, the new law creates a one time $250 rebate for beneficiaries whose costs for Part D prescription drugs exceeds the coverage gap threshold
Eventual Elimination of the • “Donut Hole” • 2010 – New law provides $250 rebate for • individuals in the “Donut Hole” • 2011 – 50% rebate will apply to brand name • prescription drugs for individuals in the “Donut • Hole” • 2020 – complete elimination of the coverage gap
What is the “Donut Hole” and How do I Know If I’ve Reached It?
Typical Medicare Prescription Drug Plan Catastrophic Coverage Plan Pays 95% Beneficiary Pays 5% $4,550.00 No Coverage “DOUGHNUT HOLE” Coverage Gap: Beneficiary Pays 100% $2,830,00 Plan Pays 75% Beneficiary pays 25% Partial Coverage
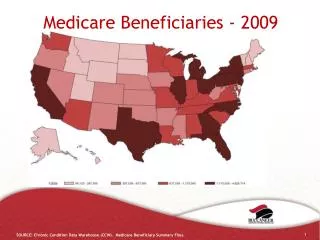
Coverage Gap Medicare Prescription Drug Plans (Medicare D Plans) have a gap in coverage sometimes called the “Donut Hole” During the Coverage Gap a beneficiary is responsible for paying 100% of their drug costs. For (2010) the Coverage Gap begins when the total cost for prescription drugs purchased through the plan reaches $2,830. The coverage gap ends when the individual’s own expenditures reaches $4,550.00. About 390,00 Medicare Beneficiaries in Pennsylvania hit the “Donut Hole” each year – the annual cost to individuals that reach the “donut hole “ averages over $4,000.
2010 Coverage Gap Rebate
$250 REBATE • For Individuals that reach the • “Donut hole” during 2010 • One time payment only • And only for 2010 year
Approximately three months after the end of the quarter • in which an individual reaches the “Donut Hole” • Medicare will automatically send out the rebate check • Quarter # 1 Ends March 31 – • Check will be mailed in June • Quarter #2 ends June 30 – • Check will be mailed in September • Quarter #3 ends September 30 – • Check will be mailed in December • Quarter #4 ends December 31 – • Check will be mailed in March
What does a qualified individual need to do to get this Rebate Check? Nothing… Qualied individuals will automatically receive their check from Medicare
How will Medicare know an individual reached the “Donut Hole”? At the end of each quarter, all insurance companies that provide Prescription Drug plans will submit a report to Medicare listing every individual that has entered the Coverage Gap during that quarter
What if I Don’t Get the Rebate Check When I Should? Contact Medicare 1-800-633-4227 Or Visit www.healthreform.gov the US government web site Managed by the Department Of Health & Human Services
Continues to close the coverage gap by reducing the percentage of cost for beneficiaries.
2011 • New Health Care Legislation will require • Pharmaceutical Manufacturers to provide • a 50% discount on prescriptions filled for • individuals in the Coverage Gap. (federal • government will provide a 7% discount on • generics for individuals in the coverage gap) • The % amount of the discount will gradually • increase each year until… • 2020 • Complete elimination of the Coverage Gap
Changes Effective In 2011 • Annual Enrollment Period (AEP) • Changes the AEP to October 15 – December 7 • Change begins October 15, 2011 • Medicare Advantage Disenrollment Period • Provides a 45 day period (1/1 – 2/15) to • Medicare Advantage enrollees, during which • time they can disenroll from Medicare • Advantage plan and return to Original • Medicare.
Changes Effective In 2011 • Physician Compare Website • Requires the Secretary of HHS to develop a • “Physician Compare” website by 1/1/2011. • Preventative Benefits • Eliminate all cost sharing for certain • preventative screening services.
Changes Effective In 2011 • Payment Rates to • Medicare Advantage Plans • Freezes payment rates for 2011 at the 2010 • payment levels • Cost Sharing Requirements • Requires Medicare Advantage plans that provide extra benefits to give priority to cost • Sharing reductions
Changes Effective In 2011 • Cost Sharing Restrictions • Prohibits Medicare Advantage plans from • imposing higher cost sharing for some • Medicare covered benefits such as • chemotherapy, dialysis, and skilled nursing • care. • Can not charge more than Original Medicare
Changes Effective In 2011 • Higher Premiums • Medicare beneficiaries with annual incomes • will pay higher Part D plan premiums • $85,000 + single • $170,000 + married • Less than 5% of the Medicare population is • subject to income-related premium • adjustments
Changes for 2012 and Beyond • Exceptions and Appeals • PDPs and MA-PDs are required to utilize a • single uniform exceptions/appeals process. • Plans are to provide instant access to the • process via the web or toll free number • Medicare Advantage Payment Rates • Reductions in payments to MA plans will be • phased in over 3 to 7 years. Plans must • still provide all benefits guaranteed by • Medicare
Changes for 2012 and Beyond • Medicare Part D Cost Sharing • Eliminates Part D cost sharing for dual • eligible beneficiaries receiving services under • a Home and Community Based Waiver • Medicare Part D Formulary • By 2014 Part D will cover Benzodiazepines • and Barbiturates
Changes for 2012 and Beyond • Nursing Home/Long Term Care Facilities • Transparency & Improvement Program • Expanding existing requirements for • Nursing/LTC facilities to provide information • to the state government on their operations: • Staff levels • Operation schedules • Wages • Organization structure • Ownership disclosure
Changes for 2012 and Beyond • Nursing Home/Long Term Care Facilities • Transparency & Improvement Program • Nursing/LTC facilities must include dementia management program following federal guidelines • Nursing/LTC facilities must provide dementia care and abuse prevention training for all existing employees and new hires • Establishes extended guidelines for national background checks for employees of Nursing/LTC facilities that have direct patient access • Nursing/LTC facilities will be required to report incidents of patient abuse