Thymoma By L.Jamal
430 likes | 831 Vues
Thymoma By L.Jamal. The Thymus. The thymus is a specialized organ of the immune system . It is located in the ant. mediastinum . Production of T- Lymphocytes. The Thymus. A pyramid shaped organ , pinkish grey in colour with a soft and lobulated surface .

Thymoma By L.Jamal
E N D
Presentation Transcript
Thymoma By L.Jamal
The Thymus • The thymus is a specialized organ of the immune system . • It is located in the ant. mediastinum . • Production of T- Lymphocytes .
The Thymus • A pyramid shaped organ , pinkish grey in colour with a soft and lobulated surface . • 5 cm in length , 4 cm in breadth and 6mm in thickness. • Wieghs 20-35 grams during puberty and regresses to 6 gr in adulthood .
Structure • 2 lobes , each lobe is composed of multiple lobules and sorrounded in a capsule . • Each lobule consists of multiple follicle. • Each follicle is divided into a capsule and medulla .
Cortex : contains thymocytes → T- lymphocytes. Medulla : contains corpuscles (area of maturation) .
Vasculature • Internal mammary , superior and inferior thyroid arteries . • The veins end in the left brachiocephalic vein (innominate vein), and in the thyroid veins .
Mediastinal Masses • Thymoma . • Lymphoma . • Germ cell tumor . • Thyroid an Parathyroid tumors .
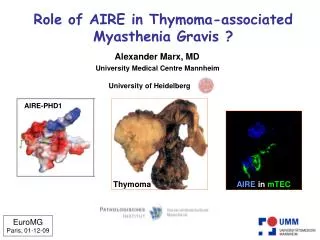
Thymoma • A neoplasm of the Thymic epithelial cells . • Results from dysregualtion of the proliferation and maturation of T- lymphocytes . • This process results in either Autoimmunity or Immune defeciency .
As a result , thymomas are associated with autoimmune diseases in 70% of the patients during diagnosis . • Thymomas are ussually encapsulated and spread by local extension .
Epidemiology • Primary tumors of the mediastinum represent 3% of all chest tumors . • Primary anterior mediastinal masses account for 50 % . • 45% are thymomas .
F:M → 1 : 1 . • Thymomas in the pediatric age group tend to run an aggressive course .
Clinical Presentation • 30 % local symptoms . • 30 % abnormal chest radiographs . • 30 % Myasthenia Gravis (paraneoplastic syndrome).
Local symptoms : Dyspnea . Dyspahgea . Cough . SVC obstruction . • Thymomas tend to be highly vascular → bleeding and necrosis .
Paraneoplastic : MG. Hypogammaglobulenemia . Good syndrome . Oppurtunistic infections .
Work up • Blood : CBC : Anaemia , thrombocytopenia , agranulocytosis . Quantitative Ig studies → Panhypogammaobulinenmia . CD4 T-cell count . Pre an post vaccination antibody levels .
Radiology : Chest x ray . CT or MRI . Nuclear imaging ( octreotide scan )
Tissue sampling : Core biopsies . FNA . Limited sternotomy Mediastinoscopy .
Histologic Findings • Mixed epithelial and lymphoid cells . • 4 categories : • Spindle cell predominant . • Lymphocyte predominant . • Mixed . • Epithelial predominant .
WHO classification : A : Spindle or Oval cells . B : dendredtic or epitheloid . AB: mixed . C : resembles other organs . • Types A , AB → benign . • Type B , C → malignant .
Staging • Masaoka Staging system . I : Macrospcopically encapsulate , no capsular invasion . II: Macroscopic invasion to surrounding tissue or microscopic capsular invasion . III : Macroscopic invasion into neighboring organs. IVa : Pleural or pericardial dissemination. IVb : Lymphogenous or hematogenous metastases
TTT • Surgical and medical . • Thymectomy is curative in the early stages . • It can be challenging . • Thymectomy releaves obstructive symptoms and improves paraneoplastic symptoms .
Hypogammaglobulinemia shows no improvement after thymectomy and requires monthly Ig infusions . • MG patients show a 25 % improvement in mw after thymectomy .
Radiotherapy : unresectable tumors & post sugical resection . • Primary radiotherapy for stages III & IVa improved the 5y survival 40-50 % . • Chemotherapy : for stages IV a , b using Cisplatin , Vincristine & Doxyrubicin .
Prognosis • Adverse predictive factors : Invasive tumor . Tracheal compression . Young age . Tumor more than 8 cm .
5 & 10 year survival • Type A - 100% and 95%, respectively • Type AB - 93% and 90%, respectively • Type B1 - 89% and 85%, respectively • Type B2 - 82% and 71%, respectively • Type B3 - 71% and 40%, respectively • Type C - 23% (5-year survival rate)
Thymic Hyperplasia • Increase in the size of the gland with normal microscopic arrangement . • Rare intety . • Presentation is similar to a thymoma .
3 subtypes : • Massive thymic hyperplasia . Common in infancy presents with compressive symptoms . • Thymic hyperplasia assocaited with endocrine abnormalities .
Rebound thymic hyperplasia : The thymus gland regresses in size during times of severe stress then enlargres beyond normal . Seen following , severe burns , pneumonia , tuberculosis and malignancies .
Management : Close monitoring for 2 years . If thymic hyperplasia doesn't regress by 2 years , biopsies and resection are warranted . rs
Thymic rebound hyperplasia in an 11-year-old girl with Hodgkin lymphoma.