Download

1 / 29
290 likes | 502 Vues
Mid- and long-term outcomes of STEMI patients treated with prasugrel , compared with clopidogrel and undergoing PCI: Observations from the TRITON-TIMI 38 trial. Elsa Margarita Arrieta, MD 1 and Hyunah Caroline Choi , MD 2. 1. Eli Lilly and Company Mexico; Mexico City, United Mexican States

E N D
Mid- and long-term outcomes of STEMI patients treated with prasugrel, compared with clopidogrel and undergoing PCI: Observations from the TRITON-TIMI 38 trial Elsa Margarita Arrieta, MD1 and Hyunah Caroline Choi , MD2 1. Eli Lilly and Company Mexico; Mexico City, United Mexican States 2 . Eli Lilly and Company Korea; Seoul, Korea Study funded by Daiichi Sankyo Company, Limited and Eli Lilly and Company.
TRITON-TIMI 38: Introduction As use of stents has grown, thienopyridines—especially clopidogrel—have become increasingly important for treatment of STEMI1-6 No randomized controlled trials have been undertaken to compare clopidogrel (or the first-generation thienopyridine, ticlopidine) with placebo in patients undergoing PCI for STEMI The effectiveness of clopidogrel in this setting has been presumed on the basis of results of studies of scheduled PCI7-9 PCI = percutaneous coronary intervention; STEMI = ST-segment elevation myocardial infarction 6Mandelzweig L et al. Eur Heart J 2006;27:2285-2293 7Mehta SR et al. Lancet 2001;358:527-533 8Steinhubl SR et al. JAMA 2002;288:2411-2420 9Sabatine MS et al. JAMA 2005;294:1224-1232 • 1Bertrand ME et al. Circulation 1998;98:1597-1603 • 2Schörnig A et al. N Engl J Med 1996;334:1084-1089 • 3Urban P et al. Circulation 1998;98:2126-2132 • 4Leon MB et al. N Engl J Med 1998;339:1665-1671 • 5Bertrand ME et al. Circulation 2000;102:624-629
TRITON-TIMI 38: Introduction cont’ Prasugrel is a novel third-generation thienopyridine and a more potent blocker of the platelet P2Y12 receptor than clopidogrel, producing consistent platelet inhibition10 The TRial to assess Improvement in Therapeutic Outcomes by optimizing platelet inhibitioN with prasugrel–Thrombolysis In Myocardial Infarction (TRITON-TIMI) 38 was designed to compare clopidogrel with prasugrel In a previous report, prasugrel was superior to clopidogrel in reduction of ischaemic events in patients undergoing PCI for the entire spectrum of acute coronary syndrome (ACS), albeit with increased bleeding11 10Wiviott SD et al. Circulation 2007;116:2923-2932 11Wiviott SD et al. Am Heart J 2006;152:627-635
TRITON-TIMI 38: Objective • To assess prasugrel vs. clopidogrel in the STEMI population • This report represents the first large experience for prasugrel in mechanical reperfusion of STEMI STEMI = ST-segment elevation myocardial infarction
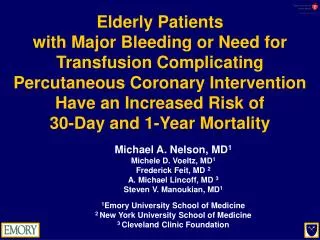
All ACS/PCI patients N = 13608 UA/NSTEMI n = 10074 Randomised patients with STEMI N = 3534 Clopidogrel 300 mg LD/75 mg MD n = 1765 Prasugrel 60 mg LD/10 mg MD n = 1769 2 patients did not receive study drug or undergo PCI Secondary PCI n = 1094 Primary PCI n = 2438 Prasugrel n = 1203 Clopidogrel n = 530 Clopidogrel n = 1235 Prasugrel n = 564 TRITON-TIMI 38: Study Design – Distribution of Patients in STEMI Cohort Double-blind, double-dummy, parallel, randomized controlled trial ACS = acute coronary syndrome; LD = loading dose; MD = maintenance dose; NSTEMI = non-ST-segment elevation myocardial infarction; PCI = percutaneous coronary intervention; STEMI = ST-segment elevation myocardial infarction; UA = unstable angina
TRITON-TIMI 38: Enrollment Criteria • Participants divided into two strata • Those enrolled within 12 hours of onset of symptoms (primary PCI) • Those enrolled between 12 hours and 14 days after onset of symptoms (secondary PCI) • Major exclusion criteria • Any thienopyridine treatment within 5 days of randomization • Need for chronic oral anticoagulants • Cardiogenic shock • Recent fibrinolytic administration • Increased bleeding risk or anaemia
TRITON-TIMI 38: Procedures • The randomization procedure was stratified by presenting syndrome (STEMI vsunstable angina [UA] or non-STEMI [NSTEMI]) • In patients with STEMI who presented within 12 hours of onset of symptoms and for whom primary PCI was planned, randomization could take place without knowledge of coronary anatomy, just after informed consent was obtained • In individuals undergoing secondary PCI, knowledge of coronary anatomy was required before randomization PCI = percutaneous coronary intervention; STEMI = ST-segment elevation myocardial infarction
TRITON-TIMI 38: Study Endpoints • Primary endpoint: cardiovascular (CV) death, non-fatal (NF) myocardial infarction (MI), or NF stroke • Key secondary endpoint: CV death, NF MI, or urgent target vessel revascularisation (UTVR) at 30 days, follow-up was out to 15 months12-16 • Other prespecified efficacy analyses included stent thrombosis (clinically adjudicated according to definite or probable Academic Research Consortium definitions)17,18 the composite of CV death or NF MI, and all individual components of the composite endpoints • Safety endpoints: thrombolysis in myocardial infarction (TIMI) major bleeding unrelated to coronary artery bypass graft (CABG) surgery, TIMI life-threatening bleeding, and TIMI major or minor bleeding unrelated to CABG surgery • Net clinical outcome endpoint: all-cause death, NF MI, NF stroke, or NF TIMI major bleeding unrelated to CABG surgery 16Antoniucci D et al. J Am Coll Cardiol 2003;42:1879-1885 17Mauri et al. N Engl J Med 2007;356:1020-1029 18Wiviott et al. Lancet 2008;371:1353-1363 • 12Brener SJ et al. Circulation 1998;98:734-741 • 13Neumann FJ et al. J Am Coll Cardiol 2000;35:915-921 • 14Montalescot G et al. N Engl J Med 2001;344:1895-1903 • 15Stone GW et al. N Engl J Med 2002;346:957-966
TRITON-TIMI 38: Statistical Analyses • The sample size for the main trial was calculated to have 90% power to detect a 20% reduction in relative risk of the primary endpoint in patients with UA or NSTEMI • The number of participants with STEMI was capped at 3500 to ensure the overall TRITON-TIMI 38 trial would have a distribution of presentations of ACS similar to that seen in the general population19 • The trial was not prospectively designed or powered to show superiority of prasugrel over clopidogrel in the STEMI cohort alone • Efficacy comparisons by time-to-first event with the intention-to-treat principle ACS = acute coronary syndrome; NSTEMI = non-ST-segment elevation myocardial infarction; STEMI = ST-segment elevation myocardial infarction; TRITON-TIMI 38 = TRial to assess Improvement in Therapeutic Outcomes by optimizing platelet inhibitioN with prasugrel–Thrombolysis In Myocardial Infarction; UA = unstable angina 19Rosamond W et al. Circulation 2008;117:e25-e146
TRITON-TIMI 38: Statistical Analyses • Safety analyses in patients who received at least one dose of study drug and in whom an event took place while on active treatment or within 7 days of treatment discontinuation • Event rates are expressed as Kaplan-Meier estimates, and estimates are compared with hazard ratios (HRs) and two-sided 95% confidence intervals (CIs) • P < 0.05 was judged significant • Numbers needed to treat and corresponding CIs were calculated with event rate estimates in the clopidogrel arm
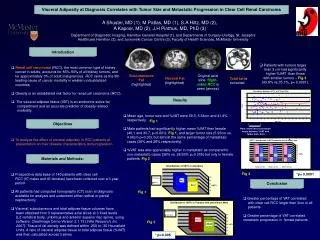
TRITON-TIMI 38: Baseline Characteristics of the STEMI Cohort – Prasugrel vs Clopidogrel IQR = interquartile range; STEMI = ST-segment elevation myocardial infarction
TRITON-TIMI 38: Baseline Characteristics of the STEMI Cohort – PrasugrelvsClopidogrel CABG = coronary artery bypass graft; IQR = interquartile range; MI = myocardial infarction; PCI = percutaneous coronary intervention; STEMI = ST-segment elevation myocardial infarction
TRITON-TIMI 38: Baseline Characteristics of the STEMI Cohort – Prasugrel vs Clopidogrel BMS = bare metal stent; DES = drug-eluting stent; PCI = percutaneous coronary intervention; STEMI = ST-segment elevation myocardial infarction
TRITON-TIMI 38: Baseline Characteristics of the STEMI Cohort – Prasugrel vs Clopidogrel GP = glycoprotein; PCI = percutaneous coronary intervention; STEMI = ST-segment elevation myocardial infarction
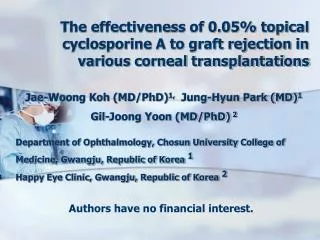
12 * Clopidogrel 10 9.5 * * 8.8 8.8 Prasugrel * 8 7.0 6.7 6.5 6.2 6 4.9 Patients (%) *p < 0.05 4 * * 2.6 2.4 1.9 2 1.6 1.3 1.2 0 CV Death/ NF MI/UTVR All-cause Death NF MI UTVR CV Death/NF MI Stent Thrombosis† CV Death/ NF MI/NF Stroke TRITON-TIMI 38: STEMI CohortEfficacyEndpointsat 30 Days †Clinically adjudicated according to definite or probable Academic Research Consortium definitions CV = cardiovascular; MI = myocardial infarction; NF = non-fatal; STEMI = ST-segment elevation myocardial infarction; UTVR = urgent target vessel revascularisation
TRITON-TIMI 38: STEMI Cohort Primary Efficacy Endpoint at 30 Days (CV Death, NF MI, NF Stroke) 15 * Clopidogrel 12.3 Prasugrel * 9.5 10 8.2 Patients (%) 6.6 6.5 6.4 *p < 0.05 5 0 All STEMI Primary PCI Secondary PCI CV = cardiovascular; NF = non-fatal; MI = myocardial infarction; PCI = percutaneous coronary intervention; STEMI = ST-segment elevation myocardial infarction
TRITON-TIMI 38: STEMI Cohort Primary Safety Endpoint at 30 Days (Non-CABG TIMI Major Bleeding) Differences between treatment groups are not statistically significant CABG = coronary artery bypass graft; PCI = percutaneous coronary intervention; STEMI = ST-segment elevation myocardial infarction; TIMI = thrombolysis in myocardial infarction
TRITON-TIMI 38: STEMI CohortEfficacyEndpointsat 15 Months 16 14 * * Clopidogrel 12.4 * 12.0 11.5 Prasugrel 12 10.0 * 9.6 10 9.0 8.8 8 6.8 Patients (%) *p < 0.05 6 4.3 * 4 3.2 3.3 2.8 2.2 1.6 2 0 CV Death/ NF MI/UTVR CVDeath/NF MI All-cause Death NF MI UTVR Stent Thrombosis† CV Death/ NF MI/NF Stroke † Clinically adjudicated according to definite or probable Academic Research Consortium definitions CV = cardiovascular; MI = myocardial infarction; NF = non-fatal; STEMI = ST-segment elevation myocardial infarction; UTVR = urgent target vessel revascularisation
TRITON-TIMI 38: STEMI Cohort Primary Efficacy Endpoint at 15 Months (CV Death, NF MI, NF Stroke) * * *p < 0.05 CV = cardiovascular; NF = non-fatal; MI = myocardial infarction; PCI = percutaneous coronary intervention; STEMI = ST-segment elevation myocardial infarction
TRITON-TIMI 38: STEMI Cohort Primary Safety Endpoint at 15 Months (Non-CABG TIMI Major Bleeding) Differences between treatment groups are not statistically significant CABG = coronary artery bypass graft; PCI = percutaneous coronary intervention; STEMI = ST-segment elevation myocardial infarction; TIMI = thrombolysis in myocardial infarction
TRITON-TIMI 38: STEMI Cohort Net Clinical Benefit at 30 Days and 15 Months * * * * * * *p < 0.05 Death/MI/Stroke/ Non-CABG TIMI Major Bleeding at 30 Days All-cause Death/NF MI/ NF Stroke/ Non-CABG TIMI MajorBleeding at 15 Months Death/NF MI/NF Stroke/ Non-CABG and CABG TIMI Major Bleedingat 15 Months MI = myocardial infarction; CABG = coronary artery bypass graft; NF = non-fatal; STEMI = ST-segment elevation myocardial infarction; TIMI = thrombolysis in myocardial infarction
TRITON-TIMI 38: Summary STEMI Cohort • Efficacy • Prasugrel: greater relative treatment effect compared to clopidogrel • Primary endpoint (CV death, NF MI, or NF stroke) significantly reduced (10.0% vs 12.4%, p = 0.02) • Safety • Prasugrel: no more significant bleeding events compared to clopidogrel • Non-CABG TIMI major bleeding (2.4% vs 2.1%, p = NS) • Life-threatening bleeding (1.3% vs 1.1%, p = NS) • Non-CABG TIMI major or minor bleeding (5.1% vs 4.7%, p = NS) NS = non-significant
TRITON-TIMI 38: Summary STEMI Cohort • Net Clinical Benefit • Outcome endpoint of all deaths, NF MI, NF stroke, or NF non-CABG TIMI major bleeding significantly favouring prasugrel both at 30 days and 15 months • Prasugrel compared to clopidogrel in patients undergoing PCI for STEMI: greater efficacy in preventing ischaemic events without an apparent increased risk of bleeding
TRITON-TIMI 38: Discussion • In STEMI patients, prasugrel compared with clopidogrel • Significant risk reduction in the primary composite endpoint of CV death, NF MI, or NF stroke for the trial duration • Significant reduction in the key secondary composite endpoint of CV death, NF MI, or UTVR at 30 days • Consistent with those of TRITON-TIMI 38, in the cohort presenting with UA or non-STEMI23,24 • TRITON-TIMI 38 was not designed or powered for all clinical endpoints in the STEMI population alone • In view of the capped sample size, we believe it is noteworthy that there was a benefit of prasugrel on ischaemic events • With a larger sample size, differences could possibly have been noted for low frequency events, including major bleeding 23Rosamond W et al. Circulation 2008;117:e25-146 24Wiviott SD et al. N Engl J Med 2007;357:2001-2015