Download
1 / 18
190 likes | 437 Vues
Two Years Safety and Efficacy of Tenofovir Disoproxil Fumarate (TDF) in Patients With HBV-Induced Cirrhosis. M Buti, 1 S Hadziyannis, 2 P Mathurin, 3 P Urbanek, 4 M Sherman, 5 S Strasser, 6 C Wang, 7

E N D
Two Years Safety and Efficacy of Tenofovir Disoproxil Fumarate (TDF) in Patients With HBV-Induced Cirrhosis M Buti,1 S Hadziyannis,2 P Mathurin,3 P Urbanek,4 M Sherman,5 S Strasser,6 C Wang,7 J Petersen,8 EJ Heathcote,9 P Marcellin,10 J Sorbel,11 E Mondou,11 J Anderson,11 and F Rousseau11 1Servicio de Medicina Interna Hepatologia, Hospital General Universitari Vall d’Hebron, Barcelona, Spain; 2Department of Medicine,Henry Dunant Hospital, Athens, Greece; 3Service d-Hepato-Gastroenterologie, Hopital Claude Huriez, CHRU Lille, Lille, France; 4Intern Klinika UVN Praha, Prague, Czech Republic; 5Toronto General Hospital, Toronto, Ontario, Canada; 6AW Morrow Gastroenterology & Liver Center, Royal Prince Alfred Hospital, Camperdown, NSW, Australia; 7Digestive Disease Institute, Virginia Mason Medical Center, Seattle, Washington, USA; 8Klinik & Poliklinik F. Innere Medizin, Universitatsklinikum Hamburg-Eppendorf, Hamburg, Germany; 9Toronto Western Hospital, University of Toronto, Ontario, Canada; 10Hopital Beaujon, Clichy, France; 11Gilead Sciences, Inc., Foster City, CA and Durham, NC, USA
Introduction • Tenofovir DF has shown maintained virologic suppression < 400 copies/mL in treatment naïve patients with chronic hepatitis B. • In an ITT analysis, 78% of HBeAg+ and 91% of HBeAg– patients maintained virologic response at week 96 in 2 pivotal studies * • Among patients remaining on treatment 89% of HBeAg+ and 99% of HBeAg– patients had HBV DNA < 400 c/mL* • Both non-cirrhotic and cirrhotic patients were enrolled in these studies allowing evaluation of the cirrhotic subset treated with tenofovir DF for 96 weeks *Marcellin et al., AASLD 2008; Heathcote et al., AASLD 2008
Objective • To evaluate the efficacy and safety of tenofovir DF among cirrhotic patients with chronic hepatitis B participating in tenofovir DF pivotal studies GS-174-0102 (HBeAg–) and GS-174-0103 (HBeAg+)
GS-174-0102 (HBeAg–) andGS-174-0103 (HBeAg+)Study Design Open-label 8 Years Double-Blind TDF 300 mg once daily (n =426*) RANDOMIZE 2:1 Tenofovir DF 300 mg once daily ADV 10 mg once daily (n = 215*) ≥ Week 72 option for FTC+TDF if viremic Week 48 Liver Biopsy† Paired biopsies in 391 TDF (92%) and 192 ADV (89%) Week 240 Liver Biopsy Pre-treatment Liver Biopsy *Combined across both pivotal studies †Open label participation gated by Week 48 biopsy Eligibility criteria required abnormal ALT, Knodell necroinflammatory score ≥ 3, and viremia with HBV DNA > 105 c/mL with the Roche COBAS TaqMan assay (LLOQ=169 c/mL [29 IU/mL]) Cirrhotics (Knodell fibrosis score=4) with compensated liver disease were eligible
Methods • Virologic response (defined as HBV DNA < 400 c/mL [69 IU/mL]) was prospectively evaluated long term (ITT) • HBV DNA and safety laboratory parameters were performed every 4 weeks (Year 1) and 8 weeks (Year 2) • For the subset analysis, the comparison of primary interest is tenofovir DF-treated cirrhotic patients versus non-cirrhotic patients through Week 96
Proportion of Patients With Cirrhosis atStudy Entry in Various Subsets • 123 cirrhotic patients were enrolled across the 2 studies • Cirrhotic patients comprised 19% of all patients • 81/426 (19%) on tenofovir DF (34 HBeAg+; 47 HBeAg– ) • 42/215 (20%) on ADV (17 HBeAg+; 25 HBeAg–) • Combined study results are presented to maximize cirrhotic patient sample size with focus on patients receiving tenofovir DF for 96 weeks 20% 19% 19% 19% 19%
Tenofovir DF Cirrhotics and Non-CirrhoticsBaseline Characteristics IQR, interquartilie range a. P-values for categorical endpoints from a Fisher's exact test. For certain endpoints the extension to Rx2 tables was used; p-values for all continuous variables calculated using a two-sided Wilcoxon Rank Sum test.
Tenofovir DF Cirrhotics and Non-CirrhoticsBaseline Characteristics (cont’d) Values are medians for continuous variables. a. P-values for categorical endpoints from a Fisher's exact test. For certain endpoints the extension to Rx2 tables was used; p-values for all continuous variables calculated using a two-sided Wilcoxon Rank Sum test.
TDF Produced Consistent HBV DNA Suppression Among Cirrhotic and Non-Cirrhotic Patients Through Week 96 < 169 c/mL (< 29 IU/mL)
ITT Proportion of Patients With/Without Cirrhosis with HBV DNA <400 c/mL (69 IU/mL) on TDF 90% vs. 85%p=0.178
On-Treatment Proportion of Patients With/Without Cirrhosis With HBV DNA <400 c/mL (69 IU/mL) on TDF 97% vs. 95%p=0.423
On-Treatment Proportion of Patients With/Without Cirrhosis With ALT in Normal Range on TDF 83% vs. 78%p=0.381 Mean ALT 34.2 & 35.2 U/L
Serology Results in Cirrhotic Patients • Among 47 HBeAg– cirrhotic patients : None lost HBsAg • Among 34 HBeAg+ patients • 2/34 (6%) lost HBsAg (both genotype D) and both seroconverted to anti-HBs (at Week 24 and 96) • one did not continue beyond year 1 (no Week 48 biopsy) • Of those with Week 96 serology results 9/29 (31%) seroconverted to anti-HBe (p=0.48 versus non-cirrhotic patients). 9/29 8/31 24/120 25/103
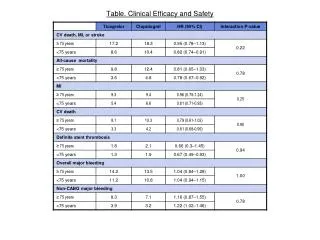
Cumulative Safety of Tenofovir DF was Not Significantly Different Among Cirrhotic and Non-Cirrhotic Patients Through Week 96 Specific Grade 3 / 4 laboratory analytes included if present in > 1 cirrhotic patient. a. P-values from a two-sided Fisher’s exact test included for combined Grade 3/ 4 AEs and labs, and SAEs.
Summary of Safety • Tenofovir DF was well tolerated in cirrhotic and non-cirrhotic patients • No patient developed decompensated liver disease or clinical evidence of impaired hepatic function while taking tenofovir DF; no cirrhotic patient died
No Resistance After 96 Weeks of TDF Monotherapy • No HBV polymerase/reverse transcriptase (pol/RT) amino acid substitutions associated with resistance to tenofovir were identified through 96 weeks of TDF monotherapy • Across both studies 24 patients had HBV DNA ≥ 400 c/mL (69 IU/mL) through 96 weeks of TDF monotherapy • 4 cirrhotic and 20 non-cirrhotic • No cirrhotic patient had virologic breakthrough • 2 cirrhotic patients had virus with no HBV pol/RT changes, one could not be genotyped, and one had polymorphic site changes
Conclusions • Tenofovir DF demonstrated potent HBV DNA suppression and good tolerability with no safety concerns in patients with compensated cirrhosis due to chronic hepatitis B • Consistent efficacy responses were observed among cirrhotic and non-cirrhotic patients treated with tenofovir DF
Acknowledgements Participating Centers US & Canada K. Hu I.Jacobson L. Jeffers K. Kaita A. Lok P. Martin T. Min R. Myers T. Nguyen P. Pockros N.Ravendhran R. Rubin V.Rustgi M. Sherman M. Shiffman M. Tong H. Trinh N. Tsai C. Wang Z. Younossi Spain, Germany & France T. Casanovas J. Enriquez G. Gerken F. Habersetzer T. Heintges C. Hezode H. Hinrichsen D. Huppe S. Kaiser M. Manns P. Mathurin S. Mauss B. Moller J. Peterson M. Prieto G. Teuber C. Trepo R. Zachoval J. Zarski S. Zeuzem UK & Netherlands R. DeMan G. Dusheiko D. Mutimer R. Williams Greece, Turkey & Italy U. Akarca P. Andreone G. Dalekos G. Germanidis S. Gurel S. Hadziyannis G. Kitis O. Kurdas S. Ozenirler M. Rizzetto H. Senturk N. Tozun Gilead Sciences J. Dinsdale A. Foster E. Montgomery S. Nonaka-Wong J. Quinn A. Snow-Lampart C. Welborn K. Washington ICON Quintiles Australia &New Zealand W.Cheng D. Crawford P. Desmond E. Gane J. George P. Gow I.Kronborg C. Moyes M. Ngu S. Roberts J. Sasadeusz W. Sievert N.Stace S. Strasser F. Weilert US & Canada N. Afdahl F. Anderson M. Bennett N. Bzowej S. Chan A. DiBisceglie P. Gaglio N. Gitlin S. Gordon J. Heathcote Bulgaria, Czech Republic & Poland R. Balabanska M. Beniowski R. Flisiak A.Gladysz W. Halota A. Horban P. Husa I. Kotzev Z.Krastev W. Kryczka T. Mach J. Sperl K. Tchernev P. Urbanek M. Volfova Spain, Germany & France K. Barange Y. Benhamou T. Berg J. Bronowicki W. Boecher P. Buggisch M. Buti J. Calleja