Download
1 / 48
480 likes | 520 Vues
Learn about opioid analgesics, their mechanism of action, therapeutic uses, side effects, and nursing implications for ensuring safe and effective pain relief. Explore opioid tolerance, dependence, and withdrawal symptoms.

E N D
Analgesics • Medications that relieve pain without causing loss of consciousness • Painkillers
Classification of Pain By Source Vascular pain • Possibly originates from vascular or perivascular tissues Neuropathic pain • Results from injury to peripheral nerve fibers or damage to the CNS Superficial pain • Originates from skin or mucous membranes
Pain Transmission Tissue injury causes the release of: • Bradykinin • Histamine • Potassium • Prostaglandins • Serotonin These substances stimulate nerve endings, starting the pain process.
Pain Transmission • These pain fibers enter the spinal cord and travel up to the brain. • The point of spinal cord entry is the DORSAL HORN. • The DORSAL HORN is the location of the “GATE.”
Pain Transmission • This gate regulates the flow of sensory impulses to the brain. • Closing the gate stops the impulses. • If no impulses are transmitted to higher centers in the brain, there is NO pain perception.
Pain Transmission • Body has endogenous neurotransmitters • Enkephalins • Endorphins • Produced by body to fight pain • Bind to opioid receptors • Inhibit transmission of pain by closing gate
Pain Transmission Rubbing a painful area with massage or liniment stimulates large sensory fibers • Result: • GATE closed, recognition of pain REDUCED • Same pathway used by opiates
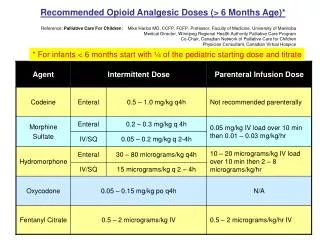
Opioid Analgesics • Pain relievers that contain opium, derived from the opium poppy or • chemically related to opium Narcotics: very strong pain relievers
Opioid Analgesics • codeine sulfate • meperidine HCl (Demerol) • methadone HCl (Dolophine) • morphine sulfate • propoxyphene HCl
Opioid Analgesics: Mechanism of Action • Bind to receptors on inhibitory fibers, stimulating them • Prevent stimulation of the GATE • Prevent pain impulse transmission to the brain
Opioid Analgesics: Therapeutic Uses Main use: to alleviate moderate to severe pain • Opioids are also used for: • Cough center suppression • Treatment of constipation
Opioid Analgesics: Side Effects • Euphoria • Nausea and vomiting • Respiratory depression • Urinary retention • Diaphoresis and flushing • Pupil constriction (miosis) • Constipation
Opiate Antagonists naloxone (Narcan) naltrexone (Revia) • Opiate antagonists • Bind to opiate receptors and prevent a response Used for complete or partial reversal of opioid-induced respiratory depression
Opiates: Opioid Tolerance • A common physiologic result of chronic opioid treatment • Result: larger dose of opioids are required to maintain the same level of analgesia
Opiates: Physical Dependence • The physiologic adaptation of the body to the presence of an opioid
Opiates: Psychological Dependence (addiction) • A pattern of compulsive drug use characterized by a continued craving for an opioid and the need to use the opioid for effects other than pain relief
Opiates • Opioid tolerance and physical dependence are expected with long-term opioid treatment and should not be confused with psychological dependence (addiction).
Opiates • Misunderstanding of these terms leads to ineffective pain management and contributes to the problem of undertreatment.
Opiates • Physical dependence on opioids is seen when the opioid is abruptly discontinued or when an opioid antagonist is administered. • Narcotic withdrawal • Opioid abstinence syndrome
Opiates Narcotic Withdrawal Opioid Abstinence Syndrome • Manifested as: • anxiety, irritability, chills and hot flashes, joint pain, lacrimation, rhinorrhea, diaphoresis, nausea, vomiting, abdominal cramps, diarrhea
Opioid Analgesics: Nursing Implications • Before beginning therapy, perform a thorough history regarding allergies, use of other medications,health history, and medical history. • Obtain baseline vital signs and I & O. • Assess for potential contraindications and drug interactions.
Opioid Analgesics: Nursing Implications • Perform a thorough pain assessment, including nature and type of pain, precipitating and relieving factors, remedies, and other pain treatments. • Assessment of pain is now being considered a “fifth vital sign.”
Opioid Analgesics: Nursing Implications • Be sure to medicate patients before the pain becomes severe as to provide adequate analgesia and pain control. • Pain management includes pharmacologic and nonpharmacologic approaches. Be sure to include other interventions as indicated.
Opioid Analgesics: Nursing Implications • Oral forms should be taken with food to minimize gastric upset. • Ensure safety measures, such as keeping side rails up, to prevent injury. • Withhold dose and contact physician if there is a decline in the patient’s condition or if VS are abnormal—especially if respiratory rate is below 12 breaths/minute.
Opioid Analgesics: Nursing Implications • Follow proper administration guidelines for IM injections, including site rotation. • Follow proper guidelines for IV administration, including dilution, rate of administration, and so forth. CHECK DOSAGES CAREFULLY
Opioid Analgesics: Nursing Implications • Constipation is a common side effect and may be prevented with adequate fluid and fiber intake. • Instruct patients to follow directions for administration carefully, and to keep a record of their pain experience and response to treatments. • Patients should be instructed to change positions slowly to prevent possible orthostatic hypotension.
Opioid Analgesics: Nursing Implications • Patients should not take other medications or OTC preparations without checking with their physician. • Instruct patients to notify physician for signs of allergic reaction or adverse effects.
Opioid Analgesics: Nursing Implications Monitor for side effects: • Should VS change, patient’s condition decline, or pain continue, contact physician immediately. • Respiratory depression may be manifested by respiratory rate of less than 12/min, dyspnea, diminished breath sounds, or shallow breathing.
Opioid Analgesics: Nursing Implications Monitor for therapeutic effects: • Decreased complaints of pain • Increased periods of comfort • With improved activities of daily living, appetite, and sense of well-being
CNS Depressants Sedatives • Drugs that have an inhibitory effect on the CNS to the degree that they reduce: • Nervousness • Excitability • Irritability • without causing sleep
CNS Depressants Hypnotics • Calm or soothe the CNS to the point that they cause sleep
CNS Depressants Sedative-Hypnotics—dose dependent: • At low doses, calm or soothe the CNS without inducing sleep • At high doses, calm or soothe the CNS to the point of causing sleep
Sedative-Hypnotics: Barbiturates Barbiturates have a very narrow therapeutic index. Therapeutic Index • Dosage range within which the drug is effective but above which is rapidly toxic.
Sedative-Hypnotics: Barbiturates Mechanism of Action • Site of action: • Brain stem (reticular formation) • Cerebral cortex • By inhibiting GABA, nerve impulses traveling in the cerebral cortex are also inhibited.
Sedative-Hypnotics: Barbiturates Drug Effects • Low doses: Sedative effects • High doses: Hypnotic effects (also lowers respiratory rate) Notorious enzyme inducers
Sedative-Hypnotics: Barbiturates Therapeutic Uses • Hypnotics • Sedatives • Anticonvulsants • Surgical procedures
Sedative-Hypnotics: Barbiturates Side Effects Body System Effects CNS Drowsiness, lethargy, vertigo mental depression, coma Respiratory Respiratory depression, apnea, bronchospasms, cough
Sedative-Hypnotics: Barbiturates Side Effects Body System Effects GI Nausea, vomiting, diarrhea Other Agranulocytosis, vasodilation, hypotension, Stevens-Johnson syndrome
Sedative-Hypnotics: Barbiturates Toxicology • Overdose frequently leads to respiratory depression, and subsequently, respiratory arrest. • Can be therapeutic: • Anesthesia induction • Uncontrollable seizures: “phenobarbital coma”
CNS Depressants: Benzodiazepines Mechanism of Action • Depress CNS activity • Affect hypothalamic, thalamic, and limbic systems of the brain • Benzodiazepine receptors
CNS Depressants: Benzodiazepines Drug Effects • Calming effect on the CNS • Useful in controlling agitation and anxiety
CNS Depressants: Nursing Implications • Before beginning therapy, perform a thorough history regarding allergies, use of other medications,health history, and medical history. • Obtain baseline vital signs and I & O, including supine and erect BPs. • Assess for potential disorders or conditions that may be contraindications, and for potential drug interactions.
CNS Depressants: Nursing Implications • Give 15 to 30 minutes before bedtime for maximum effectiveness in inducing sleep. • Most benzodiazepines (except flurazepam) cause REM rebound and a tired feeling the next day; use with caution in the elderly. • Patients should be instructed to avoid alcohol and other CNS depressants.
CNS Depressants: Nursing Implications • Check with physician before taking any other medications, including OTC medications. • It may take 2 to 3 weeks to notice improved sleep when taking barbiturates. • Abruptly stopping these medications, especially barbiturates, may cause rebound insomnia.
CNS Depressants: Nursing Implications • Safety is important • Keep side rails up • Do not permit smoking • Assist patient with ambulation (especially the elderly) • Keep call light within reach • Monitor for side effects
CNS Depressants: Nursing Implications • Monitor for therapeutic effects • Increased ability to sleep at night • Fewer awakenings • Shorter sleep induction time • Few side effects, such as hangover effects • Improved sense of well-being because of improved sleep