Download

1 / 25
270 likes | 1.24k Vues
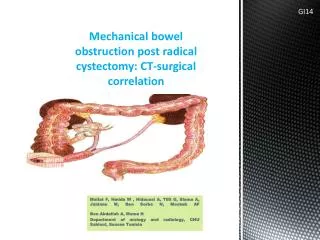
NEW APPROACH TO ACUTE BOWEL OBSTRUCTION BY MULTIDETECTOR CT. A. SAIDANE*, A. DAGHFOUS*, M. FRIKHA*, S. FELAH*, A. ZOGHLEMI**, L. REZGUI MARHOUL* Radiology* and General surgery** services Trauma center, 1007 Tunis, Tunisia. GI24. INTRODUCTION.

E N D
NEW APPROACH TO ACUTE BOWEL OBSTRUCTION BY MULTIDETECTOR CT A. SAIDANE*, A. DAGHFOUS*, M. FRIKHA*, S. FELAH*, A. ZOGHLEMI**, L. REZGUI MARHOUL* Radiology* and General surgery** services Trauma center, 1007 Tunis, Tunisia GI24
INTRODUCTION • Bowel obstruction is a leading cause of admission in surgical and emergency units. • A correct assessment of its severity, mechanism and causes is of primary importance in its management. • The multidetector CT is the main tool to achieve this purpose. • Our aim is to review the CT semiology and the different etiologies of acute bowel obstruction.
MATERIALS & METHODS • A retrospective study of 30 patients admitted from 2008 to 2011 in the service of general surgery for acute bowel obstruction. • All were explored by a 16 bars abdominal CT. • The acquisition volume goes from diaphragm to pubis with slices of 5 mm thickeness • A first spire is performed without contrast then a second one is made at a portal time (60 to 70 sec)
MATERIALS & METHODS • High intestinal opacification in 4 cases • Low intestinal opacification in 24 cases • Reconstruction in sagittal and coronal plans • 10 have evolved under suction • 20 patients were operated and a confrontation with surgical data was systematic
RESULTS About 60% of all cases wereinvolved in a smallbowel obstruction Small bowel occlusion: distendedloops ( ) with air-fluidlevels ( ) nearbycollapsed ( )or normal-caliberloops ( ) withvisualization of a transition point
RESULTS Somesigns made the obstruction’sleveldiagnosiseasier !!! Small bowelfecessign: colonicfecesappearancefound in the smallbowel String of pearlssign
RESULTS The mostcommon cause wasadhesion in patients withsurgicalhistory Beaksign: a beakformending of a distensedloop ( > )associated to a flat aspect of the loopcomingafter ( )
RESULTS Small bowel volvulus wasfound as a complication of adhesion and its main CT findingwas the Whirlsign Whirlsign: a twisting of the mesentericvasculature
RESULTS n cases of smallbowelcarcinoma: n carcinoidtumor + n adenocarcinoma Heterogenous mass of the smallbowellwitharterialenhancement Carcinoidtumor Irregularstenosiswithheterogenousthickening of the bowelwall Adenocarcinoma
RESULTS Crohndiseasewassuspected in 4 cases Coronal reconstruction: Regularstenosis of the last ilealloop ( ) Sclerolipomatosis ( ) Crohndisease
RESULTS Adenocarcinomawas the main cause of colonic obstruction Short irregular transverse colon stenosisseen in axial and sagittal reconstruction Irregularstenosis of the recto-sigmoidjunction
RESULTS Women, 65 yearsold, bowel obstruction and pain in the LIF Diverticularsigmoiditis
RESULTS Only one case of bowel obstruction wasrelated to an ileussecondary to acute appendicitis
DISCUSSION • In case of bowel obstruction, CT has to answer 5 questions: • Is that a true obstruction or not? • What is its mechanism (functional or mechanical)? • What is its level (small or large bowel)? • Is there signs of severity? • Is there an evident cause?
DISCUSSION • The positive diagnosis is based on the visualization of an intestinal distension greater than 25 mm for the small bowel and 50 mm for the colon proximally to normal-caliber or collapsed loops distally [1,2,3]. • Functional obstruction, due to a reflex ileus, results in “hydro-pneumatic” levels that are rare, diffuse with predominance of gas images while a mechanical one leads to concentrated levels around the site of occlusion
DISCUSSION • To put in evidence the level of occlusion, it is traditionally recommended to find the transition point between flat and distended intestine by following the digestive tract retrogradely departing from the rectum. • That point of transition often described as a beak sign (as it ressembles a beak) make the diagnosis much more certain [4] • We may also use other CT signs as the feces sign and the string-of-pearls sign which are related to small bowel obstruction
SEVERITY DIAGNOSIS • The sensitivity of contrast-enhanced CT for intestinal ischemia has been reported to be as high as 90% [5]. • There are various signs that have been associated with ischemia: • Thickened bowel wall : a sign of a limited value [6] • Ascites • Target sign, a trilaminar appearance of the bowel wall : very specific but rare [6] • Poor or absent enhancement of bowel wall on IV contrast-enhanced scans • Pneumatosisintestinalis • Gas in mesenteric or portal veins • Increased attenuation of bowel wall on noncontrast scan
SEVERITY DIAGNOSIS • The pneumoperitoneum signs bowel perforation which is the final stage of intestinal ischemia • Besides when the occlusion is due to a strangulation, the intestinal ischemia risk increases • CT signs of strangulation [1]: • Whirl sign, a twisting of the mesenteric vasculature signifying a volvulus • Tortuousengorgedmesentericvessels • Mesenterichemorrhage
CAUSES OF SMALL BOWEL OBSTRUCTION STRANGULATION OF SMALL BOWEL[8]: • Adhesion (70% of all SB obstruction[7]: The diagnosis is made when the patient has a surgical history and when all other causes of obstruction have been ruled out at CT (NB: do not forget that there is inflammatory, congenital and unexplained causes of adhesions). • Small Bowel Volvulus: a circumferentiallythickenedloopassociated to a whirlsign • Hernia: CT is useful in depicting the precise site and type of hernia and its contents, including spigelian, obturator, lumbar, and ventral hernias [8]
CAUSES OF SMALL BOWEL OBSTRUCTION EXTRINSIC MASSES[8]: • Carcinoidtumors: primarily intrinsic lesions of the ileum; but small bowel obstruction due to desmoplastic mechanisms operating in the mesentery which appears in CT as a nodular mass in association with retraction of surrounding bowel loops • Lymphoma: espacially the non Hodgkin nodular form that arise in the mesentery • PeritonealCarcinomatosisomental mass in the transition zone causing obstruction
CAUSES OF SMALL BOWEL OBSTRUCTION INTRINSIC MASSES[8]: • Adenocarcinoma: usually manifests at an advanced age as mural thickening with luminal narrowing at the transition zone. CT also provides information about tumor extension & distant metastases. • Crohn disease: in its advanced stenotic phase • Tuberculosis: regional nodes + thickenned bowel wall • Others: radiation enteropathy, intramural hematoma
CAUSES OF SMALL BOWEL OBSTRUCTION INTUSSUSCEPTION: • Occlusive by both a strangulation and obstuctionmechanism • Secondary to intramuralpolypoidtumors in adults • Sausage-shapedsign and targetsign INTRAMURAL CAUSES:Bezoars (intraluminalheterogenous mass), gallstones, foreign bodies, retained meconium, or tangles of ascarides INTESTINAL MALROTATION: • CT findingsincluderight-sided small bowel, left-sided colon, abnormal relationships between superior mesenteric vessels, and aplasia of the uncinateprocess. • Obstruction by smallbowel volvulus
CAUSES OF COLONIC OBSTRUCTION OCCLUSIVE CANCER:[2] 70% of cases Short stenosis without major overhauls of the pericolic fat DIVERTICULAR SIGMOIDITIS: 7% of cases Important pericolic inflammatory infiltration with or without diverticula COLONIC STRANGULATION: • Volvulus of the sigmoid: Beak sign and Whirl sign • Caecalvolvulus: 1% of cases COLORECTAL ENDOMETRIOSIS: a CT tumoral syndrom
CONCLUSION • The diagnosis of bowel obstruction is based on a comprehensive approach that includes clinical background, patient history and conventional radiography. • However, the ability to determine the site, level, cause, and severity of bowel obstruction with CT makes this modality an important additional diagnostic tool.
REFERENCES S. Nicolaou, B. Kai, S. Ho, Jenny Su, K. Ahamed.Imaging of Acute Small-Bowel Obstruction. AJR 2005; 185: 1036–1044 2) M. Deneuville, S. Beot, F. Chapuis, Ch. Bazin, H. Boccaccini, D. Regent. Imagerie des occlusions intestinales aiguës de l'adulte. Traité de Radiodiagnostic IV - Appareil digestif : 33-710-A-10 (2004) 3) K. Lebbar, D. Bassou, M. Drissi, T. Amil, M. Benameur. Les occlusions intestinales chez l’adulte: Intéret de la tomodensitométrie. Med Maghreb 2001; 87: 21-25 4) Furukawa A, Yamasaki M, Furuichi K, et al. HelicalCT in the diagnosis of small bowel obstruction. RadioGraphics2001; 21:341–355 5) Maglinte DDT, Heitkamp DE, Howard TJ, et al. Current concepts in imaging of small bowel obstruction. RadiolClin North Am 2003; 41:263–283 6) M. Zalcman, M. Sy, V. Donckier, J. Closset, D. Van Gansbeke. Helical CT Signs in the Diagnosis of Intestinal Ischemia in Bowel Obstruction. AJR 2000;175:1601–1607 7) Burkill GJC, Bell JRG, Healy JC. The utility of computed tomography in acute small bowel obstruction. Clin Radiol 2001; 56:350–359 8) M. Boudiaf, Ph. Soyer, C. Terem, J. Pelage, E. Maissiat, R. Rymer. CT Evaluation of Small Bowel Obstruction. RadioGraphics 2001; 21:613–624