Download
1 / 250
2.5k likes | 2.76k Vues
CELL ADAPTATION, INJURY AND DEATH By Larry Nichols, MD. TYPE OF NECROSIS DETERMINES TREATMENT Liquefactive: Drainage Caseous: Anti-fungal and –TB Gangrenous: Amputation. HIGH “LIVER FUNCTION TESTS” REFLECT INJURY, NOT FUNCTION Double misnomer: “LFTS” are

E N D
CELL ADAPTATION, INJURY AND DEATH By Larry Nichols, MD
TYPE OF NECROSIS DETERMINES TREATMENT Liquefactive: Drainage Caseous: Anti-fungal and –TB Gangrenous: Amputation
HIGH “LIVER FUNCTION TESTS” REFLECT INJURY, NOT FUNCTION Double misnomer: “LFTS” are neither specific for liver nor tests of function
ISCHEMIA = REVERSIBLE CELL INJURY Infarction = irreversible cell necrosis due to ischemia not relieved in time
METAPLASIA = REPLACEMENT OF A TISSUE TYPE BY ANOTHER ONE, FULLY DIFFERENTIATED BUT NOT NORMAL FOR THE SITE = a breeding ground for cancer
PATHOLOGIC APOPTOSIS Important in certain cancers chemotherapy radiation transplant rejection
Fundamental Vocabulary Etiology = doctorspeak for “cause” Morphology = pathologistspeak for “visible manifestation” Gross = pathologistspeak for “visible without a microscope”
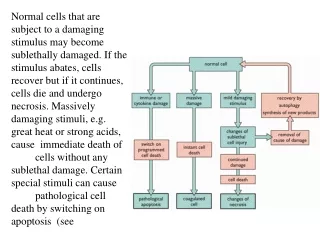
Spectrum of Cellular Responses to Stress and Noxious Stimuli ADAPTATION - INJURY - DEATH Adaptation = physiologic and morphologic changes, modulating cell function, bringing it to a new altered steady state of homeostasis
Injury = reversible pathophysiologic and morphologic response to stress or noxious stimulus exceeding cell capacity to adapt, but not enough to kill it
Cellular Adaptations Hypertrophy - Atrophy increase in cell size decrease (+/- organ size) in same Hyperplasia increase in cell number All can be physiologic or pathologic
Metaplasia = replacement of a tissue type by another one, fully differentiated but not normal for the site, pathologic Examples: replacement of bronchial respiratory epithelium by squamous epithelium due to smoking replacement of esophageal squamous mucosa by intestinal type epithelium due to reflux
Metaplasia commonly caused by processes leading to cancer Examples: gastroesophageal reflux leading to intestinal metaplasia “Barrett esophagus” leading to adenocarcinoma of esophagus smoking leading to bronchial squamous metaplasia leading to squamous carcinoma
Causes of Cell Injury Hypoxia (deficiency of oxygen) Ischemia (deficiency of blood) Physical agents (trauma, burns, etc.) Chemical agents (alcohol, drugs, etc.) Infectious agents (bacteria, etc.) Immunologic reactions Genetic derangements Nutritional imbalances
Mechanisms of Cell Injury Depletion of ATP Impaired cell surface sodium pump (sodium influx, potassium efflux) Cellular swelling Anaerobic glycolysis Impaired calcium pump (calcium influx) Reduction in protein synthesis
Mechanisms of Cell Injury Unfolded protein response Mitochondrial permeability transition (loss of cytochrome c) Activation of ATPases, phospholipases, proteases, endonucleases by calcium Accumulation of free radicals (lipid peroxidation of membranes, oxidation of proteins, DNA breaks)
Mechanisms of Cell Injury Defects in membrane permeability (mitochondrial dysfunction, cytoskeletal abnormalities, leakage from lysosomes, detergent effect of degraded membrane phospholipids, loss of membrane phospholipids)
“LFTs” slang jargon for “liver function tests” usually include bilirubin, alkaline phosphatase (“alk phos”), alanine aminotransferase (“ALT”, “SGPT”) and aspartate amino- transferase (“AST”, “SGOT”) Elevated alk phos, ALT & AST are exceedingly imperfect measures of liver injury, and not at all of function
True Liver Function Tests 1. Albumin (sometimes low level due to low liver production) 2. Prothrombin time [INR] (commonly prolonged due to hepatic coagulopathy) 3. Glucose (sometimes low level due to deficient hepatic gluconeogenesis) 4. Ammonia [NH3] (high level correlates with hepatic encephalopathy) 5. Bilirubin (sometimes)
Coagulative necrosis = morphological manifestation of irreversible cell injury (cell death) due to ischemia except in brain Liquefactive necrosis = necrosis with conversion of solid tissue to liquid due to severe acute infection, toxicity or (brain only) ischemia
Key point: ischemia is reversible (for 3 minutes in brain, for 20 minutes in heart, for 2 hours in liver) Ischemia not relieved in time causes irreversible cell necrosis = INFARCTION
Coagulative necrosis: features Preservation of ghost cell outline Cytoplasm: increased pink eosinophilia Nucleus: pyknosis (increased blue basophilia and shrinkage) karyorrhexis (fragmentation) karyolysis (fading away) Acute inflammatory response
Caseous necrosis = distinctive form of coagulative necrosis grossly resembling cheese Gangrene = distinctive form of coagu- lative necrosis with blackening and shrinkage, typically of distal extremity Fat necrosis = digested by pancreatic lipase, chalky white saponification
Type of necrosis determines treatment: Liquefactive: drainage (surgery) Caseous: anti-TB and anti-fungal Gangrene: amputation (surgery)
PATHOLOGIC APOPTOSIS Important in Certain cancers (not too many) Chemotherapy Radiation (and heat) Transplant rejection Hypoxia Certain viral infections
APOPTOSIS versus NECROSIS single cells or large groups small clusters of cells cell membrane intact disrupted inflammatory response yes no
STEATOSIS (fatty change) Abnormal accumulation of lipid in hepatocytes Due to obesity, alcohol, diabetes mellitus, anoxia, protein malnutrition
HEMOSIDEROSIS Accumulation of hemoglobin- derived, refractile, large, granular brown iron pigment Due to recent bleeding, hemolysis or iron overload “secondary hemochromatosis”
HEMOCHROMATOSIS Accumulation of hemosiderin in liver, heart, pancreas, joints and endocrine organs Due to a genetic disease causing excess dietary iron absorption “primary hemochromatosis”
LIPOFUSCIN Wear-and-tear (aging) pigment, intracellular insoluble small granular brown material composed of lipids & phospholipid polymers complexed with protein
CALCIFICATION Dystrophic: abnormal localized deposition of calcium salts in injured, dying or dead tissues Metastatic: abnormal deposition in otherwise normal tissues due to hypercalcemia, usually due to deranged calcium homeostasis
INFLAMMATION-1 By Larry Nichols, MD
ACUTE INFLAMMATION: 4 CARDINAL SIGNS & SYMPTOMS Redness Swelling Heat Pain
NEUTROPHILS: Polymorphonuclear leukocytes (“polys”, “PMNs”) Granulocytes with neutral granules, variably shaped 3- to 5-lobed nuclei First responder phagocytes
IMPORTANT MEDIATORS OF INFLAMMATION Histamine, NO, PAF, arachidonic acid, thromboxane, prostacyclin, TNF, IL-1, IL-8, interferon-g, VEGF, selectins, ICAM-1, VCAM-1, integrins, CD31, CD44, complement C3a and C5a, bradykinin, thrombin, XIIa, leukotriene B4, Toll-like receptors, G-protein receptors, serotonin, chemokines, substance P, prostaglandinD2, E2 & F2alpha
STEROIDS BLOCK PRODUCTION OF ARACHIDONIC ACID, PROSTA- GLANDINS AND LEUKOTRIENES Non-steroidal anti-inflammatory drugs block only prostaglandin production
MANY IMPORTANT MEDIATORS OF INFLAMMATION ARE ALSO IMPORTANT MEDIATORS OF BLOOD CLOTTING Mess with these important mediators of inflammation and you are messing with blood clotting.
INFLAMMATION: Complex reaction to injurious agents consisting of (1) vascular responses (2) leukocyte migration and activation (3) systemic effects
ACUTE INFLAMMATION: Rapid onset (seconds to minutes) Short duration (minutes to a few days) Exudation of fluid, plasma proteins and leukocytes (primarily neutrophils)
ACUTE INFLAMMATION: 4 CARDINAL SIGNS & SYMPTOMS Redness Swelling Heat Pain
EXUDATE: Inflammatory extracellular fluid with high protein content, cells and cellular debris TRANSUDATE: Thin serous fluid with low protein content and few (if any) cells
PUS: Purulent exudate rich in neutrophils, cellular debris and (commonly) microbes Thick, opaque, variably colored (light green, yellow, tan, crème, off-white)
NEUTROPHILS: Polymorphonuclear leukocytes (“polys”, “PMNs”, “segs”) Granulocytes with neutral granules (neither blue or red on smear), and variably shaped nuclei, segmented into 3 to 5 lobes First responder phagocytes
NEUTROPHILS: Very short-lived (1-2 days) Normally 40-70% of the leukocytes in the blood Bands: immature (adolescent) neutrophils, with nuclei with 2 lobes normally 0-5% of blood leukocytes
ACUTE INFLAMMATION: CAUSES 1) infection 2) tissue necrosis 3) immune reaction 4) trauma 5) foreign bodies 6) physical & chemical agents
ACUTE INFLAMMATION: VASCULAR RESPONSES 1) vasodilatation 2) increased permeability LEUKOCYTE MIGRATION 1) margination 2) rolling 3) adhesion 4) diapedesis 5) chemotaxis
ACUTE INFLAMMATION RECEPTORS P-selectin Rolling* # ^ E-selectin Rolling, adhesion* # ^ L-selectin Adhesion* # VCAM-1 Adhesion# ^ VLA-4 integrin Adhesion^ ICAM-1 Adhesion, diapedesis* # ^ PECAM Diapedesis *polys #monos ^lymphs
LEUKOCYTE ACTIVATION Cytokine (response and secretion) Phagocytosis(recognition, attachment*, engulfment, killing#, degradation) * greatly enhanced by opsonins # hydrogen peroxide, myeloperoxidase
CONGENITAL LEUKOCYTE DEFECTs Leukocyte adhesion deficiency-1 and -2 Chronic granulomatous disease Myeloperoxidase deficiency Chediak-Higashi syndrome
ACQUIRED LEUKOCYTE DEFECTS Diabetes mellitus Hemodialysis Malnutrition Leukemia
IMPORTANT MEDIATORS OF INFLAMMATION Histamine, NO, PAF, arachidonic acid, thromboxane, prostacyclin, TNF, IL-1, IL-8, interferon-g, VEGF, selectins, ICAM-1, VCAM-1, integrins, CD31, CD44, complement C3a and C5a, bradykinin, thrombin, XIIa, leukotriene B4, Toll-like receptors, G-protein receptors, serotonin, chemokines, substance P, prostaglandinD2, E2 & F2alpha