Bleeding disorders
Bleeding disorders. Doc. MUDr. L. Boudová, Ph.D. . Bleeding disorders I. Vessels - increased fragility II. Platelets - deficiency or dysfunction III. Coagulation disorders IV. Combination I-III. I. Vessels infections, drugs (hypersensitivity)

Bleeding disorders
E N D
Presentation Transcript
Bleeding disorders Doc. MUDr. L. Boudová, Ph.D.
Bleeding disordersI. Vessels - increased fragilityII. Platelets - deficiency or dysfunctionIII.Coagulation disordersIV.Combination I-III • I. Vessels • infections, drugs (hypersensitivity) • poor vascular wall: Ehlers-Danlos, scurvy; Cushing syndrome, old people • hereditary hemorrhagic teleangiectasia • amyloid
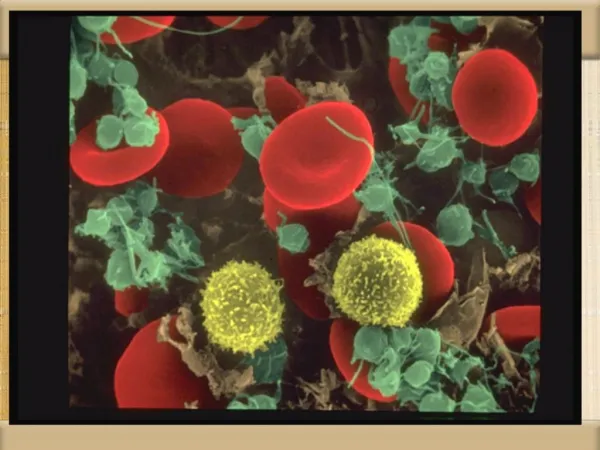
Thrombocytes 150-300 000/mm3 normal 100 000/mm3 thrombocytopenia 50 000/mm3 posttraumatic bleeding 20 000/mm3 spontaneous bleeding
Thrombocytopenia • decreased production • increased destruction • sequestration • dilution
Splenomegaly a sign of an underlying disease a problem per se bigger spleen~ bigger function = destruction of blood cells Hypersplenism • splenomegaly • (pan) cytopenia • correction of blood cytopenia by splenectomy
Immune thrombocytopenic purpura Idiopathic TP – but autoimmune! Antibodies against platelets Primary or secondary
ITP • Acute – children • Abrupt onset, both sexes, 2 weeks after virosis, resolves within 6 mo, 20% chronic • Chronic – adults (F:M 3:1) • Petechial hemorrhages and ecchymoses • Easy bruising, skin, mucosa, nose, gums, soft tis., melena, hematuria, menstruation • Clin.: nonspecific – reflective of thrombocytopenia
ITP - organs • Spleen - normal size • PB: megathrombocytes • BM:+ /- more megs • Therapy: splenectomy
Thrombotic microangiopathiesrelated clinical syndromesthrombotic thrombocytopenic purpura (TTP)hemolytic-uremic syndrome (HUS)ENDOTHELIAL INJURYWIDESPREAD HYALINE MICROTHROMBI OVERLAP - common features (TTP, HUS): • thrombocytopenia • microangiopathic hemolytic anemia • fever
Thrombotic microangiopathiesthrombotic thrombocytopenic purpura (TTP)hemolytic-uremic syndrome (HUS) Versus Disseminated intravascular coagulation Common: hyaline thrombi !!Differences:DIC: primary importance: activation of clotting system
Thrombotic microangiopathiesrelated clinical syndromesthrombotic thrombocytopenic purpura (TTP)hemolytic-uremic syndrome (HUS)ENDOTHELIAL INJURYWIDESPREAD HYALINE MICROTHROMBI OVERLAP - common features (TTP, HUS): • thrombocytopenia • microangiopathic hemolytic anemia • fever
Thrombotic microangiopathies TTP neurological deficits (transient) renal failure adult women • HUS • mostly no neurol. sympt. • acute renal failure DOMINANT! • children; E. coli O157:H7, verotoxin Common: thrombocytopenia, microangiopathic hemolytic anemia, fever
Microangiopathic hemolytic anemia hemolytic-uremic syndrome several fragmented red cells
Thrombotic microangiopathiesthrombotic thrombocytopenic purpura (TTP)hemolytic-uremic syndrome (HUS) Versus Disseminated intravascular coagulation Common: hyaline thrombi !!Differences: DIC: primary importance: activation of clotting system
Disseminated intravascular coagulation (DIC) • secondary complication of some serious condition • consumption coagulopathy • thrombohemorrhagic diathesis • acute, subacute, chronic
DIC: thrombotic andhemorrhagic diathesis activation of coagulation sequence Microthrombi hypoxia,infarctions Consumption →depletion of platelets and clotting factors + secondary activation of fibrinolysis hemorrhages
Mechanisms of DIC trigger1. Release of tissue factor or thromboplastic substances2. Widespread endothelial injury
DIC 1.obstetrics – 50%; abruptio placentae, retained dead fetus, septic abortion, amniotic fluid embolism, toxemia 2. neoplasms – 30%; adenocarcinomas, AML 3. infections – gram-negative sepsis 4. trauma, burns, extensive surgery 5. Other – snakebite, heat stroke, giant hemangioma, aortic aneurysm etc.
DIC • Morphology microthrombi • Kidneys hemorrhages Microinfarcts, bilat. renal necrosis • lungs • Brain - microinfarcts, hemorrhage • Placenta • Spleen , liver • Endocrine organs: pituitary, adrenals
DIC - clinical • microangiopathic hemolytic anemia, RDS – dyspnea, cyanosis • neurologic symptoms, oliguria, acute renal and circulatory failure, • Convulsions, coma • SHOCK
Disseminated intravascular coagulation hyaline thrombi