Download
1 / 12
120 likes | 227 Vues
The Impact of Volume of Outpatient Surgical Procedures on Quality Outcomes: 1997-2004. AcademyHealth: June 4, 2007. Research Team. Askar Chukmaitov, M.D., Ph.D. Nir Menachemi, Ph.D., M.P.H. Steven Brown, M.S. Charles Saunders, Ph.D. Robert Brooks, M.D., M.B.A.

E N D
The Impact of Volume of Outpatient Surgical Procedures on Quality Outcomes: 1997-2004 AcademyHealth: June 4, 2007
Research Team • Askar Chukmaitov, M.D., Ph.D. • Nir Menachemi, Ph.D., M.P.H. • Steven Brown, M.S. • Charles Saunders, Ph.D. • Robert Brooks, M.D., M.B.A. • Funding support from the Florida Agency for Health Care Administration (AHCA)
Rationale for the Study • Inverse relationship between hospital/surgical volume and adverse patient outcomes in inpatient settings • Better outcomes for high-volume hospitals and high-volume surgeons • Lack of research on volume-quality relationship in outpatient surgical settings • Important issue, because: • 60-70% of all surgeries are performed now in outpatient settings • Medicare payment for outpatient procedures has doubled over the last decade
Design Longitudinal analysis of 1997-2004 data Data Ambulatory discharge, hospital discharge, vital statistics Sampling Colonoscopies (n=2,820,769), Cataracts (n=2,058,090), and upper gastrointestinal endoscopies (n=1,348,121) in ASCs and HOPDs Analytical Approach Physician volume and patient outcomes (Model 1) Outpatient facility volume and patient outcomes (Model 2) Combined surgeon and facility volume and patient outcomes (Model 3) Controls: Patient severity, age, gender, payer type, location of care, time fixed effects, and clustering of outcomes Methods
Key Variables • Adverse patient outcomes • 7- and 30-day unexpected hospitalization • 7- and 30-day mortality • Physician and Facility Volume • Ranked providers according to volume tertiles: low (<34%), medium (34-67%) and high (>67%, the reference group) • Patient Severity/Risk Adjustment • Relative Risk Scores calculated using DCG/HCC methodology
Results – Descriptive • Physicians: 2,857 • Facilities: 874 (ASC=61.64%) • Unexpected Hospitalizations less than 5% • Mortality Rates less than 1% • Patient demographics • Age: 65.62 (sd=14.26) • Female: 57.3% • White: 76.79% • Severity risk score: 0.89 (sd=0.82) • Private-pay: 25.92% • Medicare: 54.56% • Medicaid: 1.95% • HMO: 13.42%
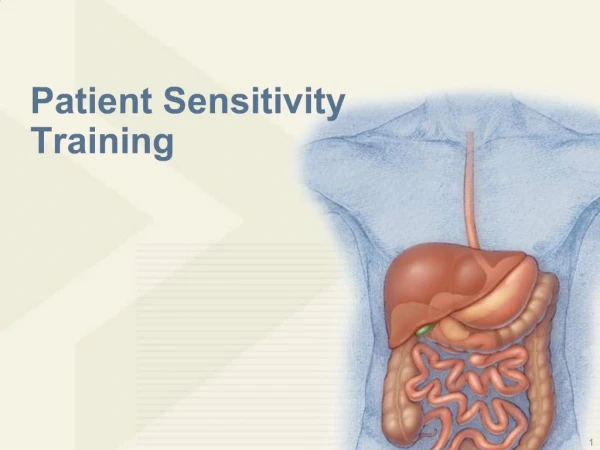
7-day Unexpected Hospitalizations after Colonoscopies *p<.05 **p<.01 ***p<.001 • Controlled for patient severity, age, gender, payer type, location of care, time fixed effects, and clustering of outcomes
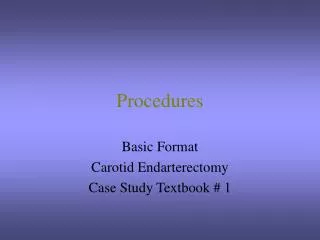
7-day Unexpected Hospitalizations after Colonoscopies *p<.05 **p<.01 ***p<.001 • Controlled for patient severity, age, gender, payer type, location of care, time fixed effects, and clustering of outcomes
7-day Unexpected Hospitalizations after Colonoscopies *p<.05 **p<.01 ***p<.001 • Controlled for patient severity, age, gender, payer type, location of care, time fixed effects, and clustering of outcomes
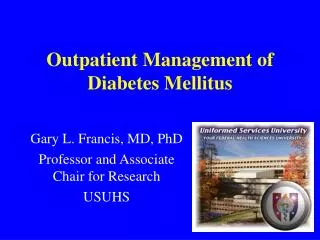
Patterns in 7- and 30-day Mortality Outcomes by Volume Category (1997-2004)
Conclusions • Consistent, dose-responsive, inverse relationship between volume and outcomes for unexpected hospitalization • Physician volume demonstrated stronger effects than facility volume • In terms of mortality, a similar pattern was noted. The lack of statistically significant findings may be due to the rarity of deaths
Significance to Policy • Further research is needed to validate these findings with data from other states, using different outcome measures, risk adjustment techniques, and analytical approaches • Volume of outpatient surgical procedures may indicate improved provider skills and processes of care delivery • Possible development of outpatient standards/guidelines (e.g., Leap Frog) • Volume-based outpatient referrals should be considered by patients, providers, payers, and policy-makers