Procedures
Procedures. Basic Format Carotid Endarterectomy Case Study Textbook # 1. Objectives. Assess the anatomy, physiology, and pathophysiology of the cerebral arterial circulatory system. Analyze the diagnostic and surgical interventions for a patient undergoing a carotid endarterectomy.

Procedures
E N D
Presentation Transcript
Procedures Basic Format Carotid Endarterectomy Case Study Textbook # 1
Objectives • Assess the anatomy, physiology, and pathophysiology of the cerebral arterial circulatory system. • Analyze the diagnostic and surgical interventions for a patient undergoing a carotid endarterectomy. • Plan the intraoperative course for a patient undergoing_____________. • Assemble supplies, equipment, and instrumentation needed for the procedure.
Objectives • Choose the appropriate patient position • Identify the incision used for the procedure • Analyze the procedural steps for carotid endarterectomy. • Describe the care of the specimen • Discuss the postoperative considerations for a patient undergoing _______________ .
Terms and Definitions • Atheroclerosis • Atheroma • Stenosis • Ischemia vs infarction • Transient Ischemic Attack (TIA)
Definition/Purpose of Procedure • Carotid endarterectomy • Removal of an atheroma from an obstructed carotid artery; the obstruction is usually at the carotid artery bifurcation • Procedure increases cerebral perfusion and decreases risk of embolization and consequent stroke
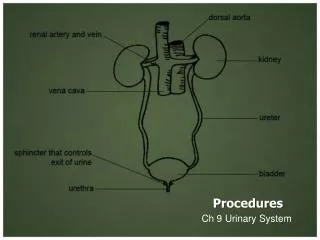
Relevant A & P • Normal cerebral blood flow
Pathophysiology: Atherosclerosis • Progressive disease characterized by atheroma, which affects the intimal and medial layers of large and midsize arteries • Caused by unknown precipitating factors that cause lipoproteins and fibrous tissue to accumulate in the arterial wall • The most accepted theory: atherosclerosis begins with an injury to or inflammation of endothelial cells lining the artery. • Endothelial damage promotes platelet adhesion and aggregation, and attracts leukocytes to the area • At the injury site: atherogenic lipoproteins collect in the intimal lining of the artery
Pathophysiology: Atherosclerosis • Macrophages migrate to the injured site as part of the inflammatory process. • Smooth muscle cells and connective tissue are stimulated to proliferate abnormally as a result of contact with platelets, cholesterol, and other blood components • Early lesion looks like a yellowish fatty streak on the inner lining of the artery • It continues to grow as a fibrous plaque and protrudes into the arterial lumen and is fixed to the inner wall of the intima and eventually occludes the vessel and affects the vessels ability to dilate in response to increased oxygen demands
Pathophysiology • Transient cerebral ischemia • TIA (Transient Ischemic Attack) • Brief period of localized cerebral ischemia causing neurological deficits lasting < 24 hrs; usually 1-2 hrs • Warning signal of ischemic thrombocytic stroke • Common S & S: contralateral weakness or numbness of hand, forearm, corner of mouth (middle cerebral artery); aphasia; visual disturbances such as blurring (posterior cerebral artery)
Pathophysiology • Thrombocytic CVA • Occlusion of a large cerebral vessel by thrombus; often in older persons who are resting or sleeping when BP is lower • Thrombi tend to form in large arteries that bifurcate; narrowed lumen as a result of atherosclerotic plaque • Common locations: internal carotid artery, vertebral arteries, junction of vertebral & basilar arteries • Occurs rapidly, progresses slowly; begins as TIA and worsens over 1-2 day period; stroke-in-evolution; when maximum neurologic deficit has been reached (3 days), called a completed stroke; damaged area is edematous, necrotic
Diagnostics • Exams • CT • Transfemoral arteriography • Trancranial ultrasound doppler • MRI • PET • LP • Preoperative Testing • Ensure that if pt is on anticoagulant therapy (ASA or Plavix, Trental, Coumadin, etc) it is discontinued a week before surgery (or as directed) • Blood work • Routine; ECG, possible chest x-ray
Surgical Intervention:Special Considerations • Patient Factors • Special consideration to compromised circulation& general state of poor vascularization (often diabetic & cigarette smokers= higher risk) • Room Set-up • Diagnostic arteriograms in the OR to view • Grafting • A Javid or Argyle shunt is frequently used for shunting cerebral blood flow & MUST BE AVAILABLE • If a graft is needed, a small portion of the saphenous vein is obtained and trimmed to size • Controversy exists r/t use of shunt • Misc • Maintain sterile set up until pt leaves room
Surgical Intervention: Anesthesia Surgical Intervention: Anesthesia • Method: General • (cervical block may be used which allows for observation of neuro changes) • Equipment • Bair hugger unit & blanket • ECG, BP, O2 Saturation • EEG (electroencephalogram) to further monitor cerebral perfusion
Surgical Intervention: Positioning • Position during procedure • Supine, head turned away from affected side about 45 degrees; neck slightly hyperextended w/roll between scalpulas; arms tucked to sides using sheet • Supplies and equipment • Small sandbag or rolled towel is placed under the shoulders to hyperextend the neck • Rest head on donut or rolled stockinette • Arm sleds to tuck and protect arms • Special considerations: high risk areas • Ulnar nerves • If a saphenous vein patch graft is to be used, the affected leg should be bent at knee and externally rotated
Surgical Intervention: Skin Prep • Method of hair removal: clipper or wet shave of leg if needed • Anatomic perimeters • From face to axillary lines; from lower ear of affected side, across midline of neck, to just below clavicle • If saphenous vein graft is to be used, also prep affected limb • Solution options • Betadine (or Duraprep) or Hibiclens
Surgical Intervention: Draping/Incision • Types of drapes: towels, laparotomy, pedi, or thyroid sheet; ¾ sheet available; may use split sheet • Order of draping • Square draping with towels and thyroid or pedi sheet • ¾ drape over feet • If saphenous vein used, place ¾ sheet under affected leg & over unaffected leg; 6 in stockinette should be rolled over the foot up to the area of the incision. A folded towel is secured over the groin; the lap, thyroid, or pedi sheet should be folded under the top of pubis • Special considerations • State/Describe incision • Incise the neck longitudinally at sternocleidomastoid muscle
Surgical Intervention: Supplies • General: lap pack or basic (thyroid drape or split), gowns/gloves, adaptic/4x4’s, lap sponges, Raytex, ESU pencil, variety of syringes & hypodermic needles • Specific • Suture & Blades: 6-0; 7-0 Prolene; 3-0, 4-0 Silk ties, 18 in.; # 11, # 10 knife blades, # 15 avail • Medications on field (name & purpose) • Heparinized NS (IV Bag) irrigation—always have available; antibiotic irrigation, Xylocaine 1% for carotid body irrigation • Catheters & Drains: typically ½ inch penrose; may use Jackson-Pratt
Surgical Intervention: Supplies • Vessel loops or umbilical tape • Suture boots • Hemostatics: Surgical, Avitene, Gelfoam • Hemoclips (sm & med) • 20-cc syringe, heparin needle or Angiocath cannula for intra-arterial irrigation • Javid or Argyle shunts (available) • Vascular patch/PFTE (Teflon) (available) • IV saline for Heparin; Bag-o-jet
Surgical Intervention: Instruments • General: Minor set, Basin set • Specific • Carotid Set • Javid shunt clamps • Hemoclip applicators (short, med, lg) • Potts & DeMartel scissors • Vascular clamps • Small nasal or neuro elevator (Penfield or Freer-type) • Yankauer suction
Surgical Intervention: Equipment • General: ESU, Suction, • Specific • Electroencephalogram (EEG)—may be used especially if no shunt used (General Anesthesia)
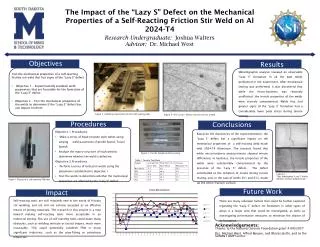
Surgical Intervention: Procedure Highlights • Neck is incised • Common, external, and internal carotid arteries are mobilized and clamped • Common carotid artery is incised • The plaque is removed • The artery is closed • The wound is closed
Neck is incisedCommon, external, and internal carotid arteries are mobilized and clamped
Common carotid artery is incised The plaque is removed Fig. 41.03b
Surgical Intervention: Procedure Steps • A longitudinal incision is made over the area of the carotid bifurcation; Weitlaner (dull) may be placed for exposure (have a variety available; sm rakes, US Army) • STSR has ready a # 10 blade w/#3 Knife handle. Place 2 folded sponges on opposite sides if the operative site. Use a magnetic pad over chest to secure instruments. • With Metz scissors, the soft tissue is dissected for exposure of the carotid artery and its bifurcation. • A moistened umbilical tape or vessel loop is passed around the vessel for traction and ease of handling. Heparin is administered systemically (per anesthesiologist).
Surgical Intervention: Procedure Steps • The common, internal, & external carotid arteries are dissected free and isolated w/vessel loops. • STSR had ready small or med Metz & sm or med Debakey forceps • Clamps are applied first to the internal carotid, then to the external carotid, then to the common carotid artery. • STSR has ready angled vascular and bulldog vascular clamps for occlusion. The internal and external carotids may be occluded w/vessel loops. NOTE TIME of heparin administration and vessel occlusion.
Restrictive Devices applied to common, external, & internal carotid arteries; See line of arteriotomy
Surgical Intervention: Procedure Steps • An arteriotomy is made over the stenotic area: the lateral portion of the distal common artery and, with the use of Potts (angulated) coronary scissors, is extended into the internal carotid artery. The full content of the occluding plaque is exposed. • STSR has ready a # 11 knife blade w/# 7 knife handle • FOR SHUNT: a piece of tubing (polyethelene or Silastic) with a suture tied around its center or commercially prepared shunt device is inserted into the common carotid artery and the internal carotid artery to maintain cerebral blood flow & is held w/vessel loops or shunt clamps
Shunt in Place:Argyle shunt is held in place with vessel loops or tapes(LT)
Surgical Intervention: Procedure Steps • The plaque is dissected free from the arterial wall, beginning in the distal common carotid artery and moving into the external & internal carotids. STSR passes blunt dissector. • A Freer elevator or # 4 Penfield dissector is used to elevate the plaque. Remaining pieces are removed with Debakey forceps and mosquito clamp. Have available Tenotomy scissors. • The endpoint is determined for the plaque in the distal internal carotid artery. The arteries are irrigated with heparinized saline to wash away any stray media or fibrin strands; to clean the intima.
Surgical Intervention: Procedure Steps • The arteriotomy is closed w/fine vascular sutures: (6-0 & 7-0 Prolene). A synthetic (polyester or PTFE) or autologous (vein) patch graft may be used to restore the arterial lumen if it is too small. • Before complete closure, blood flow is temporarily restored thru the arteries to wash away any free plaques, air, or thrombi. For this to be done, the occluding clamps are opened and closed individually, with flushing any debris away from the internal carotid artery. Surgeon checks for leaks and may repair using additional suture &/or use topical agents such as Surgicel.
Surgical Intervention: Procedure Steps • Before closure is completed, the shunt clamp or vessel loop on the internal carotid artery is released and the shunt removed. The external carotid occluding clamp is removed, followed by the common carotid artery clamp, and last, the internal carotid artery clamp • Additional interrupted sutures to control leakage • A drain is placed and secured • ½ inch Penrose is common—ensure it is secured w/ safety pin. With this drain, apply bulky 4 x4 dressings for fluid absorption • Wound is closed w/absorbable suture (4-0 Vicryl or Dexon) or staples
Counts • Initial: Sponges, Sharps • First closing • Final closing • Sponges • Sharps
Dressing, Casting, Immobilizers, Etc. • Types & sizes • 4x4 ‘s • Type of tape or method of securing • Surgeon pref: silk, cotton, etc.
Specimen & Care • Identified as atherosclerotic plaque • Handled: routine
Postoperative Care • Destination • PACU: Pt’s neurological status is carefully monitored for postop changes • Flexion and turning pt’s head are avoided to decrease risk of kinking artery, bleeding, or thrombosis; elevate HOB 20 degrees • Expected prognosis (Good, Depends on other chronic disease processes eg: HTN, recent MI, Organ dysfunction) • Discharge first postop day usually
Postoperative Care • Potential complications • Hemorrhage • Infection • Other: Stroke, Embolus, MI, Cranial nerve injury, Hematoma • Surgical wound classification: I • Type of surgery: ablative
Resources • L & B pp. 1308-1319; pp. 808-0810 • Fuller p 530 • STST: Procedure 23-6; pages 959-963 • Alexander’s pp. 1106-1109 • MAVCC Unit 13 • Complete Review of Surgical Technology by Boegi, Rogers, McGuiness • Taber’s 19th edition • AST Exemplar (handout) • www.allrefer.com
Which medication is commonly given IV about 3-5 minutes prior to cross-clamping the artery during arteriotomy? • Epinephrine • Protamine sulfate • Papaverine • heparin
The removal of plaque and removal of the lining of an artery is called a(n): • Profundoplasty • Endarterectomy • Phlebography • Arteriovenous Fistula formation
The scissors used for intravascular access during an endarterectomy are called: • Jameson • Metzenbaum • Tenotomy • Potts
_________________ is the medication used to reverse the initial anticoagulant therapy during vascular surgery: • Sodium bicarbonate • Heparin sodium • Vitamin K • Protamine sulfate
The retraction of fine sutures during vascular surgery is accomplished by the use of: • Senn retractors • Vessel loops • Malleable ribbon retractors • Penrose drain
The procedure which may require the temporary use if an intraoperative bypass shunt is a (n): • Femoral – Popliteal Bypass Graft • Abdominal Aortic Aneurysmectomy • Carotid Endarterectomy • Aortic-Artery Bypass Graft