Download
1 / 6
70 likes | 279 Vues
Patient Interested? & complex?. Stop. Implement Coordinated Care Plan. Evaluate the Process. Repeat Cycle. Revise/Modify the CCP. Evaluate The patient’s CCP. Coordinated Care Plan Process – South East LHIN Health Links. Project Manager (PM) or Care Coordinator (CC) Notified. No.

E N D
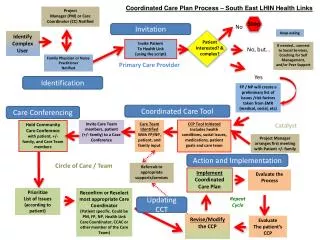
Patient Interested? & complex? Stop Implement Coordinated Care Plan Evaluate the Process Repeat Cycle Revise/Modify the CCP Evaluate The patient’s CCP Coordinated Care Plan Process – South East LHIN Health Links Project Manager (PM) or Care Coordinator (CC) Notified No Invitation Keep asking Identify Complex User Invite Patient To Health Link (using the script) If needed… connect to Social Services, Coaching for Self Management, and/or Peer Support No, but… Family Physician or Nurse Practitioner Notified Primary Care Provider Yes Identification FP / NP will create a preliminary list of issues /risk factors taken from EMR (medical, social, etc) Coordinated Care Tool Care Conferencing Invite Care Team members, patient (+/- family) to a Case Conference Care Team Identified With FP/NP, patient, and family input CCP Tool Initiated Includes health conditions, social issues, medications, patient goals and care team Catalyst Hold Community Care Conference with patient, +/- family, and Care Team members Project Manager arranges first meeting with Patient +/- family Action and Implementation Circle of Care / Team Referrals to appropriate supports/services Prioritize List of Issues (according to patient) Reconfirm or Reselect most appropriate Care Coordinator (Patient specific. Could be PM, FP, NP, Health Link Care Coordinator, CCAC or other member of the Care Team) Updating CCT
Identification • Who identifies? Variable: Physicians, clinical staff, NP, community pharmacists • Process: Data set created by hospital and clients chosen by HLs; professional network; CDR records; SE CCAC data; • Criteria for complexity: admission data - # episodes, duration; ER visits - # episodes; complex med condition i.e. CHF; at-risk of frequent and prolonged admissions; client resides in HL geography • Timeframe used for data: past 2 years (24 months); - rolling timeframe or static? 11-12 hospital data set • Things to try next: SHIIP; expand populations of interest; potentially expanding role of identification to community service providers
Invitation • Who invites? Variable: Physicians, clinical staff; NPs/Social worker; • Process: physician determines interest and if yes, the care coordinator does the consent process; standard consent form used; standard script for invitation available for suggested use • Tried in past but not continuing : not formalizing inviting them in the process but initiating the process while CHF client is hospitalized (no time to complete prior to discharge) • Things to try next: no responses here
Coordinated Care Tool • Who: physicians, RNs; RNs who are in the care coordinator positions; NPs; social worker; • Process: clinical visit, MRP segways into conversation with patient and/or family member • Site: homeor office • Version used: # 8 up to Dec; #12 – December on; #15- January on • Latest Version Available: Version #16 as of Feb 27th, 2014 • Where kept? Variable: embedded into EMR; scanned into EMR; paper copy on chart; paper copy to patient • # visits to complete CCT: usually 1 but sometimes 2 (advanced directive questions difficult to complete in the first visit) • CCAC involvement? Where indicated; little; some HLs tracking the percentage of clients with a completed CCT who have received CCAC services at the time the CCT was done • Who updates? MRP; How often updated? As required; not happening; • What have you tried in the past but not continuing? Interviewing couples together • What are you planning on trying next? Nothing at this time
Care Conferencing • Who is responsible for arranging? MRP; Care Coordinator; haven’t had any • Process: - team decides if conference is necessary; • Tried in past but not continued: may be hard to organize, but experience shows that it is not always hard to do • Try in future: how determine who needs a care conference, and how to involve CCAC care coordinators; leverage use of OTN; increase primary care provider participation; engage community partners to engage in the care conference; standardize data collection (who came to the conference, where to keep the notes from the care conference, etc) • Who essential to attend? Patient, family (if patient requested), primary care clinical staff, community agencies and other specialists • How determine who is essential? Team consensus - individualistic; • Timeframe from CCT initiation to care conference? Not sure because haven’t done one yet. Goal – hold within 14 days • Things to consider: what defines a care conference? Who defines care conference definition (Patient? Provider?) Multiple sectors? Multiple providers?
Action and Implementation Who carries out the action/implementation of the plans arising from care conference? MRP; whoever was assigned the task Process: not determined/articulated yet Updating Who is responsible for updating the CCT? NPs; other? Process for updating: In one FHT, the NPs update in the EMR and the CCT is populated automatically (some parts); other?