Download
1 / 27
270 likes | 668 Vues
Presentation. 34 year old female with a history of hypothyroidism presents with abdominal pain, weakness, night sweats, fevers and weight loss.15 lb unintentional weight loss over 6 weeksFevers to 101?Recent drenching night sweatsDiffuse moderate abdominal pain. HPI. 5-6 weeks of progressive dif

E N D
1. Pancytopenia and �B� Symptoms in a Previously Healthy Female
Robert J. Hoffman MD
December 20, 2006
2. Presentation 34 year old female with a history of hypothyroidism presents with abdominal pain, weakness, night sweats, fevers and weight loss.
15 lb unintentional weight loss over 6 weeks
Fevers to 101�
Recent drenching night sweats
Diffuse moderate abdominal pain
3. HPI 5-6 weeks of progressive diffuse abdominal pain
Waxes and wanes
Better with food
Moderate severity
New DOE restricting her activity as well
Recent diagnosis of Barrett esophagus
4. PMH Hypothyroidism
Barrett esophagus based on recent EGD
GERD
5. Medications Prilosec
Synthroid
OCP
6. Social History No tobacco, alcohol or illegal drug use
Single
Works as an accountant
7. Physical Examination Vitals: T: 98.5 P: 98 RR: 16 BP: 109/41
General: Comfortable appearing, pale, NAD
Abd: soft, moderate epigastric and RUQ tenderness. No organomegaly
No LAD
Otherwise normal exam.
8. Labs
9. 10mm, 8mm, 4mm liver lesions
5 x 3 cm pelvic mass
Small amount of pelvic ascites CT Abdomen
10. Initial Hospital Course MRI orderd to f/u pelvic mass.
Hematology consult obtained, bone marrow biopsy planned for Monday.
PRBC transfusion
Haptoglobin < 6, consistent with hemolysis
LDH elevated
11. Hospital Course MRI reveals pelvic �mass� to be an enlarged vaginal vault.
u/s fails to confirm liver nodules
Decreased bone marrow signal found on MRI c/w marrow replacement
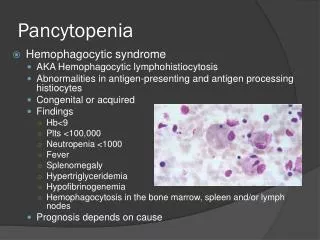
12. Summary Pancytopenia
�B� symptoms
Abdominal pain
Decreased marrow signal
Intravascular hemolysis
13. Phew! B12 returns 78 pg/ml
Homocysteine and methylmalonic acid elevated
Anti-parietal cell antibody positive.
B12 supplements initiated
Bone marrow shows hypercellularity and erythroid hyperplasia, consistent with vitamin B12 deficiency
14. Outcome At one week follow up patient states she �feels better than she has in years�
Hemoglobin was 9.2 g/dl on d/c and 11.8 g/dl at one week follow up.
Other cytopenias resolve.
15. Pernicious Anemia Autoimmune disorder with T-cell mediated immune response to intrinsic factor and gastric parietal cells
Atrophic gastritis
Achlorhydria
16. Autoimmune Disorders Hashimoto�s thyroiditis
DM I
Celiac sprue
17. B12 Deficiency Megaloblastic anemia
Leukopenia
Thrombocytopenia
Peripheral neuropathy
Psychosis, personality changes, memory loss
19. Other Findings Ineffective erythropoiesis ? mild hemolysis
Achlorhydria
Elevated gastrin
Adenocarcinoma and carcinoid tumors
Atrophic glossitis
20. Diagnosis Low B12 OR Low Normal B12 with elevated MMA/homocysteine
Elevated intrinsic factor ab, anti-parietal cell antibody, elevated gastrin
Atrophic gastritis on EGD
Schilling test
21. Treatment Historically treatment is with IM B12
Recent data suggests po a reasonable alternative
Second pathway for B12 absorption without intrinsic factor
22. Treatment Small 1998 study randomized pt�s to cobalomin 1 mg IM at scheduled intervals vs. daily 2mg orally
Higher B12 and lower MMA levels in oral group than IM group at 120 days f/u
Only 33 patients
Only 7 with clear pernicious anemia
23. Treatment 60 patients with megaloblastic anemia randomized to 1g IM vs. 1g po daily for 10 days followed by once/wk followed by monthly
Hgb, B12, retic, MCV increased in both groups similarly
In patients with neurologic deficits, 78% improved in IM vs. 75% in po
Small study, etiology of deficiency not fully tested
24. Treatment PO therapy a reasonable alternative.
Some experts recommend initial IM therapy, especially in the presence of neurologic symptoms.
PO therapy standard of care in Canada and Sweden.
25. Classic Case? Pancytopenia
Hemolysis
Peripheral smear
Glossitis (maybe)
26. Incongruities Barrett esophagus in a patient with achlorhydria?
�B� symptoms
27. Take Home Points Think of B12 deficiency in patients with cytopenias (not just anemia!), neurologic dysfunction.
Confirm with B12 +/- MMA & homocysteine.
Oral therapy is probably preferred.