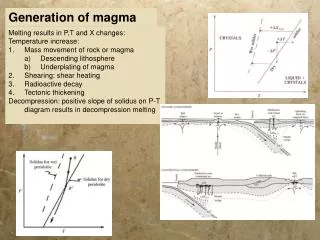
X STOP ™ Interspinous Process Decompression (IPD ® ) System
X STOP ™ Interspinous Process Decompression (IPD ® ) System. Marco Artiano, M.A. Chapman University Doctor of Physical Therapy Program July 2008. FDA Approval?. FDA Approved 11/21/05 St. Francis Medical Technologies, Inc. Address: 960 Atlantic Avenue, Suite 102 Alameda, CA 94501

X STOP ™ Interspinous Process Decompression (IPD ® ) System
E N D
Presentation Transcript
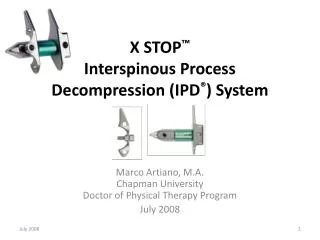
X STOP™Interspinous Process Decompression (IPD®) System Marco Artiano, M.A.Chapman University Doctor of Physical Therapy Program July 2008
FDA Approval? • FDA Approved 11/21/05 • St. Francis Medical Technologies, Inc.Address: 960 Atlantic Avenue, Suite 102Alameda, CA 94501 • http://www.fda.gov/cdrh/pdf4/p040001a.pdf
What is X STOP? • The X STOP ® Interspinous Process Decompression System (aka “X STOP”) is used to relieve symptoms of lumbar spinal stenosis. The X STOP® is a titanium implant that fits between the spinous processes of the (lumbar) spine. It is made from titanium alloy and consists of two components: a spacer assembly and a wing assembly. • How does it work? The X STOP® implant is placed between the spinous processes of the symptomatic lumbar levels. The X STOP® is designed to limit extension of the spine in the affected area, which may relieve the symptoms of lumbar spinal stenosis.
X STOP™ - Indications for use • The X STOP® implant is indicated for treatment of patients aged 50 or older suffering from pain or neurogenic intermittent claudication in the legs secondary to a confirmed diagnosis of lumbar spinal stenosis. The X STOP® is indicated for those patients with moderately impaired physical function who experience relief in flexion from their symptoms of leg/buttock/groin pain, with or without back pain, and have undergone a regimen of at least 6 months of nonoperative treatment. The X STOP® may be implanted at one or two lumbar levels. • What will it accomplish? The X STOP® may relieve some or all of the symptoms of lumbar spinal stenosis and may improve a patient’s ability to function.
X STOP™ - Indications for use • Neurogenic Intermittent Claudication (NIC: leg, buttock, or groin pain that is relieved when the spine is flexed such as when sitting in a chair), due to Central and/or Lateral-Recess Lumbar Spinal Stenosis. • Spondylolisthesis up to grade 1.5 /4 (~35%), with NIC. • Baastrup’s Syndrome / ‘Kissing Spine’. • Axial-load induced back pain. • Facet Syndrome. • Degenerative and/or Iatrogenic (post-discectomy) Disc Syndrome. • Contained HNP. • Unloading of disc adjacent to a Lumbar Fusion Procedure, primary or secondary.
XSTOP® Contraindications The X STOP® should not be used in patients with: • An allergy to titanium or titanium alloy • Spinal anatomy or disease that would prevent implantation of the device or cause the device to be unstable in the body: • significant instability of the lumbar spine • an ankylosed segment at the affected level(s) • acute fracture of the spinous process or pars interarticularis • significant scoliosis • Neural compression causing neurogenic bowel or bladder dysfunction; • Diagnosis of severe osteoporosis • Active systemic infection or infection localized to the site of implantation. http://www.fda.gov/cdrh/pdf4/p040001.html
X STOP™- Surgical Technique • Safe and accurate / No risk to neural elements • Can be performed under local anesthesia • Performed as same-day or short-stay routine http://www.kyphon.com/sfmt/press/xstop.html
X STOP™- Surgical Technique http://www.sfmt.com/sfmteuro/indications.html
X STOP ™ - Unloads It unloads: • Posterior annulus pressure by avg. of 63% • Posterior nucleus pulposus pressure by avg. of 41% • Facet force by avg. of 68% http://www.sfmt.com/sfmteuro/indications.html
XSTOP ™ Benefits • Anatomical structures: • Supraspinous ligaments • Interspinous ligaments • No bone-removal: • Direct decompression is not required • Modification of the spinous processes and/or lamina is not required • Kinematics: • Extension is limited, flexion remains unchanged • Lateral bending and axial rotation remain unchanged
XSTOP ™ Benefits • Sagittal Alignment: • Increases disc height • Restores sagittal balance • Forward bending by patient no longer necessary • Patients resume normal posture • Preserves Treatment options: • All alternative surgical options are still open; all of the original anatomy is intact
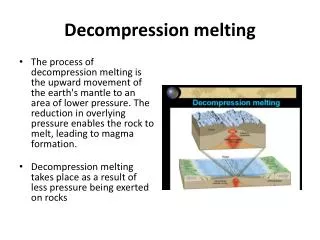
X STOP™ Decompresses • The dimensions of the spinal canal and lateral neural foramen change significantly with posture. • In a degenerated spinal segment, extension can cause anatomic structures to compress the spinal cord and/or nerves, leading to various symptoms including neurogenic intermittent claudication (NIC).
X STOP™ Decompresses • The XSTOPPK™ significantly prevents narrowing of the spinal canal and neural foramina in extension, decompressing the individual degenerative spinal level(s) that provokes symptoms.
XSTOP™ Functional Benefits • X STOPPK is designed to relieve the patient’s symptoms while standing and walking, which allows the patient to resume their normal posture.
XSTOP™ - Postoperative Care • Ambulation begins immediately after recovery and the patient is usually discharged one to two hours after the procedure. • Shower and drive a car the following day. • Apply an ice pack. Non steroidal anti-inflammatory drugs (ANSAIDs) are prescribed and mild analgesics and muscle relaxants as needed. • Return to usual activities in 10 -14 days. • No heavy labor or prolonged sitting. • Mild progressive exercise program can begin the day after the surgery. • Walking- as tolerated but not to exceed one hour in duration. • After two weeks, cycling as tolerated. • Physical Therapy is recommended for the first several weeks following surgery to condition the patient and to allow the patient's spine to adjust to the implant. • Gradual physical activity, with progression is recommended for the first 6 weeks. • Avoid hyperextension of the spine • No heavy lifting, no stair climbing, no sports such as swimming, golfing, tennis, racquetball, running or jogging. This will avoid damage to the spinal processes. • Strenuous activities and swimming may be added at six months. • A stress fracture of the spinal process may occur if strenuous physical activity is resumed too soon postoperatively.
Studies: The X STOP May Reduce Neurogenic Claudication in Lumbar Spinal StenosisSpine. 2005;30:1351-1358 • Patients were at least 50 years old and had leg, buttock, or groin pain. All were able to walk at least 50 feet. Patients with a fixed motor deficit, cauda equina syndrome, previous lumbar surgery, or spondylolisthesis of more than grade 1 were excluded from the research protocol. • Patients were randomized to receive either conservative therapy or X STOP. Those in the conservative therapy group all received at least 1 steroid injection along with analgesics and physical therapy as necessary. • Study participants were examined at 6 weeks, 6 months, 1 year, and 2 years for the main study outcomes. Outcomes were drawn from the Zurich Claudication Questionnaire and included measurements of symptoms and physical function. Patient satisfaction and radiographic changes were also assessed. • 191 patients were randomized from 9 U.S. centers. The mean age was 69 years, and baseline symptoms and physical function were similar between the 2 treatment groups. Spondylolisthesis of grade 1 or less was present in approximately one third of the cohort. • In the X STOP group, 100 patients received implants at 136 levels. The average procedure time was 54 minutes, and 97 of the procedures were completed under local anesthesia. The control group received a total of 216 epidural steroid injections during the study period. • The X STOP group performed significantly better in the main study outcomes. This improvement was evident at 6 weeks and remained static during the rest of the trial period. At 2 years, the mean improvement in symptom severity was 45.4% in the X STOP group, compared with 7.4% in the conservative management group. Improvements in physical function were 44.3% and -0.4%, respectively. • Rates of clinically significant improvement in symptoms and physical function in the X STOP cohort were 60.2% and 57%, respectively. The respective values for the conservative management group were 18.5% and 14.8%. • 73.1% of participants in the X STOP group reported being at least somewhat satisfied with treatment, compared with 35.9% of the conservative therapy group. This difference was also significant. • Factors associated with a better outcome with X STOP were the absence of comorbid conditions and lower surgical blood loss. In contrast, a positive femoral stretch test was associated with worse outcomes in the X STOP cohort. • Rates of decompressive surgery were 26.4% in the conservative therapy group and 6% in the X STOP group. • Radiographic measurements were similar between groups at 12 and 24 months. • No device-related intraoperative complications were reported with X STOP. There were 3 reports of complications associated with X STOP surgery, and 3 participants reported device-related complications during the follow-up period. In comparison, there were 5 complications associated with epidural injection. http://www.medscape.com/viewarticle/507174_print
Studies: High failure rate of the interspinous distraction device (X-Stop) for the treatment of lumbar spinal stenosis caused by degenerative spondylolisthesis. Verhoof, OJ, Bron , LJ, Wapstra, FH, van Royen BJ.Eur Spine J (2008) 17:188–192 • A cohort of 12 consecutive patients with symptomatic lumbar spinal stenosis caused by degenerative spondylolisthesis were treated with the X-Stop. • All patients had low back pain, neurogenic claudication and radiculopathy. MRI of the lumbosacral spine showed a severe stenosis. • 10 patients the X-Stop was placed at the L4–5 level. 2 patients were treated at both, L3–4 and L4–5 level. • The mean follow-up was 30.3 months. • Recurrence of pain, neurogenic claudication, and worsening of neurological symptoms was observed in three patients within 24 months. Post-operative radiographs and MRI did not show any changes in the percentage of slip or spinal dimensions. • Finally, secondary surgical treatment by decompression with posterolateral fusion was performed in seven patients (58%) within 24 months.
XSTOP™ - The Surgeryby John C. Chiu, M.D., D.Sc, F.R.C.SDepartment of Neurospine SurgeryCalifornia Center for Minimally Invasive Spine SurgeryCalifornia Spine Institute Medical CenterJohn C. Chiu: Treatment Of Lumbar Spinal Stenosis With Interspinous Process Decompression System (IPD) (X-Stop®): The Internet Journal of Minimally Invasive Spinal Technology. 2007; Volume 1, Number 1.
XSTOP™ - The Surgery • Anesthesia • The surgeon may typically use monitored IV conscious mild sedation combined with local anesthesia, allowing a greater selection of higher anesthesia risk patients for this IPD procedure. In this manner, the anesthesiologist or the anesthetist can administer 2 g of Ancef and 8 mg dexamethasone IV at the start of the procedure. Local anesthesia of 1% Xylocaine mixed with 0.25% Marcaine is injected into subcutaneous tissue and paraspinal tissue. The patient should be sedated but remain awake and responsive to verbal commands (conscious sedation). Patients should not be disoriented. • The use of surface EEG monitoring provides added precision of anesthesia delivery, and offers an additional safeguard for patients undergoing this IPD procedure.
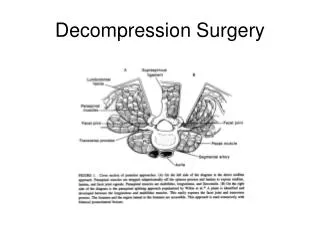
XSTOP™ - The Surgery • Skin incision and localization • After the surgical field is prepped and draped, a 4-8 cm. vertical midline lumbar incision is made over the proper spinal processes, under fluoroscopic guidance. • Using an 18 gauge spinal needle, the intraspinal process space for IPD insertion can be identified fluoroscopically. • Of course, the skin and fascia are infiltrated on both sides of the supraspinous ligament, leaving 1.5 cm. of ligament width intact . Also posterior rami nerves along the posterior aspect of facets joints and pars are infiltrated. A retractor is placed in after subperiosteal dissection of the tissue.
XSTOP™ - The Surgery • Creating the pilot hole • After incision of the lumbar fascia on either side of the spinal processes and supraspinous ligament, the dissection of the paraspinal muscle is performed, separating the bony spinal processes and lamina. The supraspinous ligament is preserved. With flexion position of the lumbar spine, the interspinous ligament is entered with a small curved dilator by paralleling the dilator to the spinous process until the facet is encountered, then rotating the instrument 90° and interspinous ligament with the tip of dilator into the lowest point of the interspinous ligament . Fluoroscopy is used to confirm the position of the dilator. A larger sized dilator is to follow to dilate the ligamentous opening further.
XSTOP™ - The Surgery • Application of the sizing distractor. • The sizing distractor is to be placed in the same opening as far anteriorly toward the lumbar lamina as possible for advancing of the distractor. A finger on the contralateral margin of the interspinous ligament to find the tip of the distractor as it passes through the opening. Once the distractor is in place, squeeze its handle gently and slowly until the resistance is encountered. As the handles are squeezed more and more, resistance should increase. When the supraspinous ligament becomes taut, optimal sizing has been achieved. Fluoroscopy is utilized for confirmation.
XSTOP™ - The Surgery • With the handles open, the tip of the sizing distractor is shaping the opening of the spacer of X-STOP® implant. The measurement of the opening for the distractor ranges from 6 mm. to 14 mm. corresponding to the size of the X-STOP® implants available. A locking nut at the base of the handle can be adjusted to fix the tips at specific size. • X-STOP implants: 6mm – 14mm sizes
XSTOP™ - Fluoroscopic Confirmation Lateral and AP views of fluoroscopic confirmation of the X-STOP implant at L4 – L5 in proper position
XSTOP™ - Two Implants • When two X-STOP® implants are placed at adjacent levels, usually there is a slight overlap of the superior and inferior implant wing with the shorter wing of the superior implant positioned posteriorly to the long tapered wing of the inferior implant. Rotation of the inferior implant wing would be effectively prevented. Again, fluoroscopy confirms the correct placement of the X-STOP's . Fluoroscopic confirmation of the X-STOP implants at L3-L4 and L4 – L5 in proper position
References • Lindsey DP, Swanson KE, Fuchs P, et al. The Effects of an Interspinous Implant on the Kinematics of the Instrumented and Adjacent Levels in the Lumbar Spine. Spine, 2003. 28(19): p. 2192-7. • Richards J, Majumdar S, Lindsey DP, et al. The Treatment Mechanism of an Interspinous Process Implant for Lumbar Neurogenic Intermittent Claudication. Spine. 2005 Apr 1;30(7):744-9. • Swanson KE, Lindsey DP, Hsu KY, et al. The Effects of an Interspinous Implant on Intervertebral Disc Pressures. Spine, 2003. 28(1): p. 26-32. • Wiseman C, Lindsey D, Fredrick A, et al. The Effect of an Interspinous Process Implant on Facet Loading During Extension. Spine. 2005 Apr 15;30(8):903-7. • Zucherman JF, Hsu KY, Hartjen CA, et al. A Multicenter, Prospective, Randomized Trial Evaluating the X STOP Interspinous Process Decompression System for the Treatment of Neurogenic Intermittent Claudication: Two-Year Follow-Up Results. Spine. 2005 Jun 15;30(12):1351-1358. • Lindsey DP, Swanson KE, Fuchs P, et al. The Effects of an Interspinous Implant on the Kinematics of the Instrumented and Adjacent Levels in the Lumbar Spine. Spine, 2003. 28(19): p. 2192-7. • Richards J, Majumdar S, Lindsey DP, et al. The Treatment Mechanism of an Interspinous Process Implant for Lumbar Neurogenic Intermittent Claudication. Spine. 2005 Apr 1;30(7):744-9. • Swanson KE, Lindsey DP, Hsu KY, et al. The Effects of an Interspinous Implant on Intervertebral Disc Pressures. Spine, 2003. 28(1): p. 26-32. • Wiseman C, Lindsey D, Fredrick A, et al. The Effect of an Interspinous Process Implant on Facet Loading During Extension. Spine. 2005 Apr 15;30(8):903-7. • Zucherman JF, Hsu KY, Hartjen CA, et al. A Multicenter, Prospective, Randomized Trial Evaluating the X STOP Interspinous Process Decompression System for the Treatment of Neurogenic Intermittent Claudication: Two-Year Follow-Up Results. Spine. 2005 Jun 15;30(12):1351-1358. • Chiu J. Treatment Of Lumbar Spinal Stenosis With Interspinous Process Decompression System (IPD) (X-Stop®): The Internet Journal of Minimally Invasive Spinal Technology. 2007; Volume 1, Number 1. • http://www.youtube.com/watch?v=cMzp4dkcSEE – a movie of the X-Stop procedure