Download
1 / 50
520 likes | 1.4k Vues
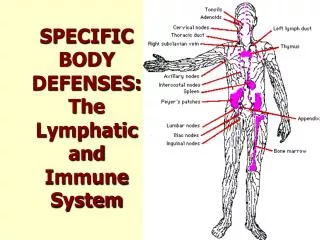
Lymphatic System and Body Defenses. Chapter 12. Lymphatic System. 2 parts Lymphatic vessels Transport back to blood, fluid escaped from CV Lymphoid tissues and organs House phagocytes and lymphocytes. Lymphatic Vessels.

E N D
Lymphatic System and Body Defenses Chapter 12
Lymphatic System • 2 parts • Lymphatic vessels • Transport back to blood, fluid escaped from CV • Lymphoid tissues and organs • House phagocytes and lymphocytes
Lymphatic Vessels • As blood circulates, hydrostatic and osmotic pressure force fluid out of arterial ends at capillary bed and in at venous ends • Fluid that remains up to 3L a day + leaked plasma proteins must be returned to blood for vascular system to function • Edema – impairs cells ability to exchange • Drainage system picks up lymph and returns to blood
Lymphatics • One way system -> heart • Blind ended lymph capillaries between tissue cells and blood capillaries in loose connective tissue, absorbed leaked fluid Figure 12.2
Lymphatic Capillaries • Very permeable • Endothelial cells loosely overlap forming minivalves • Collagen fibers anchor to CT • Open when interstitial fluid pressure greater, fluid enters lymphatics • Close when pressure in lymphatic capillary, forces lymph along capillary • Anything can enter!! • What’s the problem? • Detours!
Lymph Transportation Figure 12.1 • From lymph capillaries to lymphatic collecting ducts to venous system by right lymphatic duct or thoracic duct • Thin walled, larger have valves • Low pressure, pumpless system, transportation same as veins + smooth muscle in larger lymphatics contract rhythmically to move Figure 12.3
Lymph Nodes – What are they? • Protection – remove foreign material, produce lymphocytes (immunity) • Lymph travels toward heart filtered by 1000’s of nodes • Large clusters found in axillary, inguinal, cervical regions • Macrophages and lymphocytes • “Swollen glands”
Lymph Nodes - Structure • Most kidney shaped • Fibrous capsule, trabeculae extend inward dividing • Internal structure of reticular CT • Outer = Cortex, follicles with dark staining center called germinal centers • Inner = Medulla, macrophages Figure 12.4
Follicles of the lymph node • Follicles contain collections of lymphocytes • Germinal centers enlarge when B cells (lymphocyte) generating daughter cells = plasma cells • T cells are other lymphocyte
Travel Through Lymph Node • Lymph enters convex side through afferent vessels • Sinuses • Exits hilum via efferent vessels • # of efferent < # of afferent, drainage slow, time for macrophages and lymphocytes to work • Can get clogged – tender or not?
Other Lymph Organs - Spleen • Blood rich, filters blood of bacteria, viruses and debris • Site for lymphocyte proliferation and surveillance • Destroys worn-out RBC, returns break down to liver – iron • Stores platelets and blood reservoir (liver) – hemorrhaging • Fetus – hematopoietic site, Adults – only lymphocytes produced
Other Lymph Organs - Thymus Gland • Over heart • Peak function in youth • Hormone Thymosin -> programming of T cell lymphocytes
Other Lymph Organs - Tonsils • Ring pharynx • Trap and remove bacteria and foreign pathogens entering throat • Can become congested with bacteria, red, swollen, sore • Part of MALT
Other Lymph Organs – Peyer’s Patches • Wall of small intestine • Macrophages • Capture and destroy bacteria before able to penetrate intestinal wall • Part of MALT – mucosa-associated lymphatic tissue • Protect upper resp. and digest. from foreign matter always entering
Body Defenses Figure 12.6 • Two systems: Innate and Adaptive Defense Systems • Innate – nonspecific, responds immediately, reduces workload of adaptive • Adaptive – specific, attack against particular invader, must be “primed”, slower but precise • Immunity = highly specific resistance to disease
Innate Body Defenses • Refers to barriers that cover body, cells and chemicals that act on initial front to protect from pathogens • Nonspecific – doesn’t distinguish between bacteria, virus, fungus, etc.
Innate Body Defenses – Surface Membrane Barriers • First Line of Defense • Skin and mucous membranes • Intact, keratinized epidermis physical barrier • Mucous membranes – line cavities open to exterior, physical barriers and secretions • Acidic pH of skin secretions (pH3-5) inhibits bacterial growth, vaginal secretions acidic • Stomach mucosa secretes HCl and protein-digesting enzymes • Saliva and lacrimal fluid contain lysozyme • Sticky mucous traps organisms in digestive and respiratory tracts • Structural elements – mucous coated cilia, respiratory
Innate Body Defenses: Internal Cells and Chemical • Second line of Defense • Phagocytes and NK cells – destructive • Inflammatory Response • Chemical Substances that kill bacteria and help repair tissue • Fever
Phagocytes • Macrophage or neutrophil engulfs foreign particle • Flowing cytoplasmic extensions bind and pull inside, enclose in vacuole • Vacuole fused with lysosome, digested Figure 12.7
Natural Killer Cells • Police blood and lymph • T cell lymphocyte, unique • Can lyse and kill cancer and viral infected cells before adaptive arm enlisted • Not specific, recognize any target by recognizing certain sugar on surface and lack of self molecules • NOT phagocytic – release lytic chemical called perforin http://www.drugabuse.gov/NIDA_notes/NNvol21N6/morphine.html
Inflammatory Response Increase blood flow to area Chemotaxis Plasma leakage from blood Figure 12.8
What is the purpose of inflammation? • Prevents spread of pathogen • Phagocytosis of pathogen • Clotting proteins, wall off area, contain and repair • Disposes of cell debris and pathogens • Neutrophils via diapedesis, enter tissue drawn by positive chemotaxis • Engulf dead damaged cells • Monocytes -> macrophages follow neutrophils • May see third line of defense if contained • Sets stage for repair • Heat increase cellular metabolism, speeds defenses and repair
Antimicrobial Proteins - Complement • 20 plasma proteins circulate in blood inactive • Bind sugars or proteins on foreign cell’s surface (Ab) • One result is MAC – membrane attack complex • Amplify inflammation response – chemicals • Vasodilators • Chemotaxis chemicals • Foreign cells sticky (opsonization) Figure 12.10
Antimicrobial Proteins - Interferon • Viral infected cells release small proteins called interferons • Diffuse to nearby cells and bind to membrane receptors • Stimulates synthesis of proteins that interfere with ability of viruses to multiply within the cell
Fever • Temp regulated by hypothalamus • Pyrogen chemicals secreted by WBC and macrophages exposed to pathogens trigger increase in temp • Mild to moderate benefit body • Bacteria need Zn and Fe to replicate, during fever spleen and liver take up • Increases metabolic rate of tissue cells, repair
Adaptive Body Defenses • Very specific immune response • Requires initial exposure to “prime” immune cells, more vigorous response second time • Third Line of Defense • Protects from many pathogens • Protects from damaged, mutated self cells • Failure leads to diseases such as • Cancer • RA • AIDS
Adaptive Body Defenses • It is antigen specific – acts/recognizes specific invaders • It is systemic – immunity not restricted to initial site of infection • It has memory – recognizes and mounts stronger attacks after initial introduction • Depends on cells ability to recognize foreign Ag and communicate with each other to mount effective response • 2 components • Humoral Immunity – Antibody • Cell Mediated Immunity – Cellular
Antigens • Ag – any substance that is capable of mobilizing our immune system and provoking an immune response • Mostly nonself • Proteins, nucleic acids, carbohydrates, lipids • Proteins strongest Ag • Something is antigenic because surface bears these molecules • Self cells also have these molecules • During maturation, lymphocytes are exposed to self molecules and don’t recognize as foreign • Highly antigenic to others though – organ donation, grafts!
Cells of Adaptive Defense:Lymphocytes • T cells and B cells • Originate in red bone marrow • When released identical, differentiation depends on site of immunocompetent Figure 12.11
T cells • Immunocompetent in thymus • Maturation takes 2-3 days, directed by thymosin • Divide rapidly • Only those recognize foreign Ag survive • Those recognize self-antigens destroyed • “Self tolerance” part of education of lymphocytes
B cells • Immunocompetent in bone marrow • Divide rapidly • Only those recognize foreign Ag survive • Those recognize self-antigens destroyed • “Self tolerance” part of education of lymphocytes
Immunocompetent Lymphocytes • Immunocompetent lymphocyte only able to recognize 1 Ag • All receptors on lymphocyte surface recognize same Ag • Become immunocompetent before meeting antigen • Genes dictate receptors on lymphocyte surface not antigens • Many types of lymphocytes will never be needed. • Migrate to lymph nodes and spleen, meet Ag, complete maturation process • Circulate through body (especially T cells)
Macrophages • Monocyte formed in bone marrow • Big eaters in innate defense • Antigen presenters to lymphocytes • Secrete cytokines (proteins) • Activated T cells release chemicals cause macrophages to become killer macrophages • Remain fixed in lymphoid tissue
Humoral (Ab-mediated) Immune Response • Immunocompetent, but immature B cell – Ag binds receptors on surface, activates, clonal selection • Clonal Selection – growth and division of B cell producing many copies of cells exactly the same, Ag-specific receptors • Clone generation - 1° humoral response Figure 12.12
Humoral Immune Response • Most clones become plasma cells • Lag period • 2000 Ab/sec • Production lasts 4-5 days • Ab levels peak at 10 days post contact, decline • Some Memory Cells • Immunological memory • 2° humoral response • Produced much faster (2Hrs), more effective • Peak 2-3 days, levels remain high weeks to months
Primary vs. Secondary Response Figure 12.13
Active vs. Passive Humoral Immunity • Active Immunity – production of Ab against Ag • Naturally acquired – during infection, develop signs or symptoms of infection • Artificially acquired – vaccines • Spare from symptoms of disease • Weakened Ag • Both prime the immune system for next exposure
Active vs. Passive Humoral Immunity • Passive Immunity • Ab from serum of an immune human or animal donor • When? • B cells not challenged by Ag, no memory • Naturally – mother to baby in breast milk • Artificially – Immune serum or gamma globulin (hepatitis) • Antivenom – snake bites • Antitoxin – botulism, rabies, tetanus • Both of these will kill someone before active immunity
Active vs. Passive Humoral Immunity Figure 12.14
Antibodies or Immunoglobulins (Igs) • Soluble proteins secreted by B cells and plasma cell offspring in response to Ag • 5 classes • Basic structure • 4 polypeptide chains • Linked by disulfide bonds • 2 light, 2 heavy chains • Variable region – Ag binding site • Constant region – determines class, roles in body, cells and chemicals can bind Figure 12.15
Antibody Classes Table 12.2
Antibody Functions • Compliment fixation – main Ab ammunition against cellular Ag, bacteria or mismatched blood cells, triggers lysis • Neutralization – Ab bind exotoxins or viruses, block harmful effects • Agglutination – more than one binding site, Ag-Ab complexes of cellular Ag, mismatched blood, blood typing • Precipitation – Ag-Ab complexes of soluble antigenic material • Agglutination and precipitation easier to catch Figure 12.16
Cell-Mediated Immune Response • Immunocompetent T cells activated by exposure to Ag • Must be “presented” Ag by antigen presenting cell like macrophage • 2 components to presentation • Antigen • Self protein on surface of cell Figure 12.17
Types of T cells – Cytotoxic T cells • Kill virus infected, cancer, foreign graft cells • Bind to foreign cell • Release toxic chemicals • Granzymes • Perforins Figure 12.18
Types of T cells – Helper T cells • Directors • Interact with Ag bound B cells, stimulate faster division, Ab production • Cytokine release • Stimulate Cytotoxic T cells, B cells • Attracting WBCs Neutrophils • Enhance phagocytic activity of macrophages
Types of T cells – Regulatory T cellsand Memory Cells • Regulatory T cells • Suppress activity of T cells and B cells • Memory T cells • Immunological memory