Download
1 / 94
940 likes | 1.16k Vues
Female Reproductive System Outline. Cervix Vulva Vagina Uterus Ovaries Breast. Female Reproductive System Outline. Cervix. Development of transformation zone. Transformation Zone. Significance: Ectropion in young women, normal Nabothian cysts because of blockade of endo-

E N D
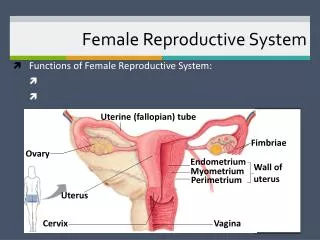
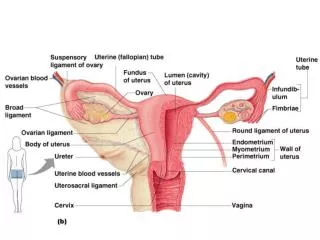
Female Reproductive System Outline • Cervix • Vulva • Vagina • Uterus • Ovaries • Breast
Female Reproductive System Outline • Cervix
Transformation Zone Significance: Ectropion in young women, normal Nabothian cysts because of blockade of endo- cervical glands Transformation zone provides a zone of immature cells which is more vulnerable to infection by HPV.Hence development of CA cervix.
Transformation zone Normal cervix, young adult
Cervicitis • Commonest organism, C.Trachomatis Others: • Ureaplasma urealyticum, T. vaginalis, Candida spp., Neisseria gonorrhoeae, herpes simplex II Clinical: • Leucorrhea • Acute and chronic inflamation • Cervical excitation tenderness(Chandelier test) Herpes simplex in pregnant women may cause fatal neonatal infection.
Cervical Carcinoma • Once the most common cancer in women – now not even in top 10. • Decrease due to Pap test in the last 50 years • At the same time, precursor lesions are increasing (early detection)
Cervical Intraepithelial Neoplasia (CIN) • Precursor to carcinoma • Almost all carcinomas arise in CIN; but not all cases of CIN progress to carcinoma! • Three grades: • CIN I: mild dysplasia (half regress, 20% progress) • CIN II: moderate dysplasia • CIN III: severe dysplasia (30% regress, 70% progress) • The higher the grade, the more likely the lesion will progress to carcinoma
Cervical Carcinoma Current grading system: Two grades. Low grade Squamous intraepithelial lesions ,LSIL(CIN I)..Rx. Observation. High grade Squamous intraepithelial lesion, HSIL(corresponding to CIN II and III)Rx. Biopsy.
normal CIN I CIN II CIN III I Cytology of CIN (Pap smear)
normal CIN I CIN II CIN III “Low-grade dysplasia” “High-gradedysplasia” Cytology of CIN (Pap smear)
Cervical Carcinoma Risk Factors • Early age at first intercourse • Multiple sexual partners • A male partner with multiple previous partners • Persistent infection with “high-risk” HPV(16=60%,18) • Smoking • Immunodeficiency
Cervical Carcinoma and HPV • HPV is detectable in almost all CIN and cancer. • “High-risk” types: • 16, 18, 45, 31 • Found in carcinomas • Integrate into genome, inactivate p53, RB • “Low-risk” types: • 6,11 • Found in condylomas (benign lesions) • Do not integrate into genome
Cervical Carcinoma and HPV • HPVs infect immature basal cells of the squamous epithelium via immature metaplastic squamous cells present at the squamocolumnar junction. • Mature superficial squamous cells that cover the ectocervix, vagina, or vulva are spared. Hence a relatively low frequency of vulvar and penile cancer compared to cancers in d cervix.
Cervical Carcinoma and HPV • Viral E6 and E7 proteins are critical for the oncogenic effects of HPV. • E6:Inactivation of P53,upregulation of telomerase. • E7: Inactivation of Rb ,up-regulation of cyclin, HPV E6 induces rapid degradation of p53 via ubiquitin-dependent proteolysis, reducing p53 levels by two- to three-fold. E7 complexes with the. • The physical state of the virus differs in different lesions, being integrated into the host DNA in cancers, and present as free (episomal) viral DNA in condylomata and most precancerous lesions.
Cervical Carcinoma and HPV • Many women with HPV never develop carcinoma.Hence other factors play a role.(Other co-carcinogens, the immune status of the individual, and hormonal factors)
Invasive Cervical Carcinoma • Most cases are squamous, arising from CIN • Small number are adenocarcinomas • Peak age: 45 (10-15 years after CIN develops!) • Spreads slowly • Most cases are diagnosed early • Mortality is related to stage: • stage 0 (preinvasive): 100% 5 year survival • stage 4: 10% 5 year survival
Cervical Carcinoma • Clinical: • Exophytic - necrotic fungating mass • Ulcerative,sometimes infiltrative tumor • 30-50 years • Irregular vaginal bleeding, post-coital bleeding • Vaginal discharge, • Pyometron due to obstruction. • Rx: Surgery +Radiotherapy.
Vulva Bartholin cyst • Acute infection of he Bartholin glands • N. Gonorheah • Edematous, painful vulva • Treatment :Marsupialization.
Vulva Non-Neoplastic Epithelial Disorders of unknown etiology. Old name Leukoplakia(white patch), Two distinct entities; • lichen sclerosus and • (2) squamous cell hyperplasia ( lichen simplex chronicus)
lichen sclerosus Etiology is unknown • Thinning of the epidermis , superficial hyperkeratosis, and dermal fibrosis with a scant peri-vascular, mononuclear inflammatory cell infiltrate • Smooth, white plaques or papules the surface resembles parchment. • Post –menopausal women. • Slightly increased risk of developing Squamous cell carcinoma
SQUAMOUS CELL HYPERPLASIA • Old names , hyperplastic dystrophy, or lichen simplex chronicus • Non- specific condition arising from frequent scratching or rubbing of the vulva • It is marked by epithelial thickening, expansion of the stratum granulosum, and significant surface hyperkeratosis.
Vulva Condylomata acuminata • Sexually transmitted infection with HPV 6 and 11 • Not associated with malignancy
Vulva Neoplasms Two group of invasive cancers: • Basaloid and warty carcinomas related to infection with high oncogenic risk HPVs (30% of cases) • keratinizing squamous cell carcinomas, not related to HPV infection (70% of cases) • Basaloid and Wart lesions occur in reproductive age women while the peak age for keratinizing squamous cell carcinoma is 76 years.
Vulva Neoplasms Basaloid and Warty cancers: • Develop from Vulva intraepithelial neoplasms,formerly Bowen disease of the vulva (VIN) • HPV 16 responsible for most lesions • Younger age group, reproductive age women.
Vulva Neoplasms • keratinizing squamous cell carcinomas • Old ,premenopausal women with history of Lichen sclerosus or squamous cell hyperplasia • No HPV infection • Chronic epithelial cell irritation
Paget disease of the vulva Intra-epithelial proliferation of malignant cells Present as • Pruritic, red, crusted, sharply demarcated, maplike area, occurring usually on the labia majora • Disease is confined to the epidermis (unlike breast paget disease where there is underlying malignancy in nearly 100%) • PAS staining would reveal the presence of PAS positive malignant cells.
Female Reproductive System Outline • Cervix • Uterus • endometriosis • endometrial hyperplasia • tumors
Endometriosis • Location of endometrial glands outside uterus • Usually peritoneum, rarely lymph nodes • Endometrium undergoes cyclic bleeding • Causes scarring, pain, sometimes sterility • How does endometrium get out?
Endometrial Hyperplasia • Proliferation of endometrium due to estrogen excess • Risk factors: anovulatory cycles, obesity, estrogen-producing ovarian tumors, exogenous hormone use • Three categories: simple, complex, and atypical • The more severe the hyperplasia, the greater the chance that it will evolve into carcinoma
Simple Complex Atypical Endometrial hyperplasia
Leiomyoma • “Fibroid” • Benign tumor of smooth muscle • Common! • Stimulated by estrogen • Menorrhagia, metrorrhagia, or asymptomatic
Leiomyosarcoma • Malignant tumor of smooth muscle • Necrotic, with atypical cells and lots of mitoses • Often recur after surgery • Many metastasize, especially to lungs • 5 year survival = 40%
Leiomyoma Leiomyosarcoma
Leiomyoma Leiomyosarcoma
Endometrial Carcinoma • Peak age: 55-65 (not before 40) • Frequently arises in endometrial hyperplasia • Risk factors: obesity, nulliparity, estrogen replacement • Symptoms: leukorrhea, irregular bleeding • Metastasizes late
Female Reproductive System Outline • Cervix • Uterus • Ovaries
Female Reproductive System Outline • Cervix • Uterus • Ovaries • Tumors
Surface epithelial tumors Germ cell tumors Sex cord-stromal tumors • Cystadenoma • Cystadenocarcinoma • Teratoma • Dysgerminoma • Yolk sac tumor • Choriocarcinoma • Granulosa-theca cell tumor • Sertoli-Leydig cell tumor Origin of Ovarian Tumors