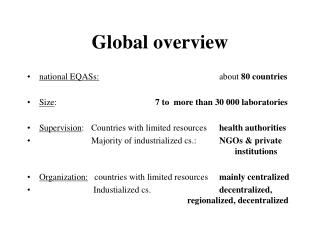
Global Overview Progress Towards Global Immunization Goals
330 likes | 599 Vues
Global Overview Progress Towards Global Immunization Goals 21 st inter-country meeting of national managers of the Expanded Programme on Immunization Cairo, 26-29 June 2004. Global Goals UNGASS, WHA, MDGs UN General Assembly Special Session (UNGASS) goals by 2010:

Global Overview Progress Towards Global Immunization Goals
E N D
Presentation Transcript
Global Overview Progress Towards Global Immunization Goals 21st inter-country meeting of national managers of the Expanded Programme on Immunization Cairo, 26-29 June 2004
Global Goals • UNGASS, WHA, MDGs • UN General Assembly Special Session (UNGASS) goals by 2010: • > 90% coverage of infants nationally & > 80% coverage in every district • Vitamin A Deficiency Elimination • World Health Assembly (WHA) resolutions & UNGASS goals by 2005: • Polio Eradication • Measles Mortality Reduction • Maternal and neonatal tetanus (MNT) elimination • Millennium Development Goal (MDGs): • 2/3rd reduction in child mortality in 2015 (compared to 1990)
DTP3 coverage by WHO Region, 1995-2002 DTP3 coverage by WHO Region, 1995-2002
Slide Date: October 03 33 million infants not immunized (DTP3), 2002 Source: WHO/UNICEF estimates, 2003
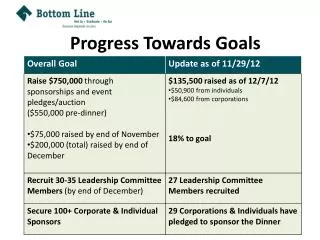
All countries (n=192) 2002 2003 reporting >80% DTP3 coverage in all districts 26% 26% countries >90% DTP3 national coverage 53% 53% 80% in all districts & 90% national: 26% 26% VF-eligible countries (n=75) reporting >80% DTP3 coverage in all districts 12% 13% plus countries >90% DTP3 national coverage 21% 21% 80% in all districts & 90% national: 12% 12% Immunizationn coverage Progress towards UNGASS goal on coverage
Recommended strategies to reach> 80% coverage in every district • Restoring outreach • Linking services and community • Monitoring and use of data for action • Managing human and financial resources • Strengthening supportive supervision
Careful planning at the local level!Map of City Neighbourhood farming area tent city factory middle class houses h.centre slum area slum area market housing dense housing footpath small road bus station boundary main road
Vaccination Delivery Strategies to Reach All Ministry of Health, Turkey
Ensuring safety Injection safety assessments Update 25 April 2004 - includes assessments done by standardized and non standardized protocolsList of countries planning injection safety assessment in 2004 is not exhaustive
Immunization safety: What is needed? • Exclusive use of vaccines of assured quality • No reuse of needles/syringes (AD syringes) • Proper disposal & appropriate waste management • Safe vaccine reconstitution and use of multi-dose vials • Effective monitoring & management of safety issues & rumours
High performing surveillance/laboratory networks Coverage monitoring that is accurate and timely Cross-checking through surveys & assessments Development of investment cases Using the data to guide policy/strategy Pursuing global immunization goalsthrough an "evidence-based" approach
The evidence…….1.4 million child deaths globally are preventable by routine vaccination, 2002 Source: WHO/IVB
Measles mortality reduction% reduction in estimated measles deaths by WHO region between 1999 & 2002
Global Measles/Rubella Laboratory Network - 2004 National Laboratories Regional Reference Labs Global Specialised Labs Proposed National Labs The designation employed and the presentation of material on this map do not imply the expression of any opinion whatsoever on the part of the secretariat of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. N=671 31 Provincial labs 326 Prefecture Labs Measles Strain Banks 154 Sub-National Labs 149 countries 160 Data as of April 2004
Laboratory network reveals a “sea of rubella” Rubella infection in first 3 months of pregnancy has a 90% risk of CRS birth defects Documented CRS incidence 0.2 to 4.3/1000 live births in non-industrialized countries (studies from 50 countries) Estimated >100,000 infants with CRS each year CRS disability (deafness, blindness, heart disease, mental retardation) is costly for families and society Compelling evidence on the burden of congenital rubella syndrome (CRS)
Countries with rubella vaccine in the national immunization system, 2003 1996 67 countries 12% of birth cohort 2003 105 countries 23% of birth cohort Source: WHO Department of Immunization, Vaccines and Biologicals, April 2004
The primary purpose of rubella vaccination is to prevent CRS Can be achieved by immunizing child-bearing aged women (CBAW) Introduce rubella vaccine into childhood immunization only if: Infant measles vaccine coverage > 80% and can be sustained Ensure immunity among CBAW Warning! Inadequate childhood rubella vaccine coverage (<80%) can: alter the transmission dynamics of rubella leading to increased susceptibility in CBAW Increase the risk of CRS WHO position paper on rubella vaccinesWeekly Epidemiological Record 2000;75:161-169
Anticipated progress by 2005 among 57 targeted countries for MNT elimination Validated countries by 2005 Countries on track for validation Countries with limited progress The boundaries and names shown and the designations used on this map do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement. Source: WHO/UNICEF MNT collected data As of 30 April 2004
Polio Progress, 2004 cases as of 22 June Paralyzed Children Asia & north Africa = 32 Sub-saharan Africa = 301 Wild virus type 1 Wild virus type 3 Endemic countries Importations
Enormous potential to contribute to MDG goals!!Causes of 4.1 million child deaths (out of 10.5 million child deaths globally)
Dare to dream!What may be possible in the next 10 years in vaccinology!
Status by end of 2003 All countries (n=192) HepB in schedule: 75% Developing countrieswith adequate delivery systems* (n=149) HepB in schedule: 85% with comparable coverage to DTP3** 42% VF eligible countrieswith adequate delivery systems* (n=61) HepB in schedule: 82% with comparable coverage to DTP3** 30% What is possible!GAVI milestoneBy 2007, all countries will have introduced hepatitis B vaccine
Slide Date: October 03 Countries having introduced Hib vaccine and reported Hib3 coverage, 2002 1997 (25 countries introduced) Hib vaccine introduced but no coverage data reported (25 countries) Hib vaccine not introduced (167 countries) 2002 (84 countries introduced (44%) Hib3 > 80% (45 countries) Hib3 < 80% (10 countries) Hib vaccine introduced but no coverage data reported (29 countries) Hib vaccine not introduced (108 countries) Source: WHO/UNICEF joint reporting form, 2002 data from 192 WHO member states
Slide Date: October 03 Countries providing vitamin A supplementationwith routine immunization services, 2002 Vitamin A distributed with routine immunization services (65 countries or 48%) Global Summary of EPI-linked VitA Distribution VitA with routine EPI: 24 countries VitA with EPI campaigns: 15 countries VitA with both (routine & EPI campaigns): 41 countries Total: 80 countries No Vitamin A distribution linked to routine immunization services (countries 71 or 52 % ) (Note: 15/71 provided vitA with immunization campaigns) Non deficient (56 countries) Source: WHO/UNICEF joint reporting form, 2002; WHO SIA database data from 192 WHO member states
R&D accelerating New partnerships Meningitis Vaccine Programme African AIDS Vaccine Programme Measles Aerosol Project GAVI-ADIPS (Rotavirus-Pneumo) Japanese Encephalitis Project [HPV/cervical cancer Vaccine] Need for consolidation (less fragmentation of various immunization initiatives) New vaccines will cost more; financial sustainability becomes paramount Vaccine supply & quality issues are more complex increased divergence of products for industrialized vs non-industrialized countries increased number of manufacturers, particularly from non-industrialized countries increased need for functional NRAs, need for new regulatory pathways Changing landscape in the immunization world
Urgency to pursue the current 2005 & 2010 goals UNGASS coverage goal will not be met unless considerable acceleration to reach every district Disease control goals (polio, measles, MNT, Vit A elim) Safety/quality is not an option, but a responsibility Enormous potential for impact with future vaccines Need strong evidence base for the old & the new Changing landscape Conclusion
Reach more Focus unprecedented attention on the "hard-to-reach" Expand to other age-groups Use school contacts Provide New Ensure the widespread use of new or under-utilized vaccines Include others Deliver additional health interventions at immunization contacts The way forwardA WHO/UNICEF Global Vision for Immunization