Download
1 / 20
220 likes | 1.33k Vues
DiNEH -- Modeling of Survey Results to Predict Medical Outcomes. Glenn Stark Johnnye Lewis Navajo Nation Human Research Review Board Conference Window Rock, AZ November 16, 2011. Funding provided by NIEHS, RO1 ES014565; R25 ES013208; P30 ES-012072; DHHS/NIH/NCRR #1UL1RR031977-01.

E N D
DiNEH -- Modeling of Survey Results to Predict Medical Outcomes Glenn Stark Johnnye Lewis Navajo Nation Human Research Review Board Conference Window Rock, AZ November 16, 2011 Funding provided by NIEHS, RO1 ES014565; R25 ES013208; P30 ES-012072; DHHS/NIH/NCRR #1UL1RR031977-01
DiNEH Project history and purpose (2000-present) • Original Goal: • ENHB’s Concern in 1990s: Does drinking uranium in unregulated water increase risk of kidney disease? • Evolved to broadly examine environmental uranium exposures and health • Community-based participatory research • Build Navajo community research capacity • Respect culture and language • Commitment to inform policy and improve clinical care • Participation in Waxman Hearing (2007), EPA Five-Year Plan • Collaboration with Navajo Area IHS medical monitoring program: Community Uranium Exposure-Journey To Healing
DiNEH Project reviewed and approved by: • Navajo Nation Human Research Review Board • UNM Human Research Review Committee • Peer-Reviewed by National Institute of Environmental Health Sciences of NIH • Data presented reflect participation and support from 20 chapters of the Eastern Agency of the Navajo Nation
Goal -- find early indicators of disease • Address barriers existing in our understanding or community uranium exposures • Develop method to assess lifespan exposures • Biomonitoring only reflects recent exposures • Environmental characterization also primarily current • Evaluate exposure within the context of existing health status and known health risk factors • Find way to improve clinical screening and policy decisions
New Hypothesis Knowledge Testing Data Collection Incorporation Model Refinement Revision Testing Iterative approach to model development • First 150 participants: • relationship between kidney disease, hypertension, and autoimmune and number of mines in each chapter • First 500 participants: • Environmental exposures to waste (in addition to known risk factors) increase the likelihood of the same diseases • First 1100 respondents: • 6 activities shown to increase risk for same diseases • First 1100 respondents: • Proximity alone was a good predictor of same diseases Diné learning model informs DiNEH research
Current models for increased disease risk combine self-reported and geospatial data • Self-reported disease diagnosis • Kidney disease • Diabetes • High blood pressure (hypertension) • Autoimmune disease • Family history of disease • Accepted risk factors for disease (age, gender, obesity) • Self-reported history of possible patterns of exposure to uranium mine and mill waste
Surrogate measures for exposure estimate life-span exposures to uranium waste • Self-reported and geospatial data are used to determine exposure • Location of home relative to abandoned mines, mills and waste piles (Mean residence is 32 years; Many have only one residence) • Environmental and occupational histories (1,304 respondents) • Exposures divided into 2 classes -- differ by dose, frequency, route ? • Active mining era -- likely higher dose, more frequent, ingestion, inhalation most likely routes, radiation more likely? • Environmental legacy (ongoing) -- lower dose, less frequent, inhalation most likely route ?
(B) and (D) (A) (B) (C) (E) Active-mining related exposures were estimated from self-reported survey data A: Washed the clothes of a uranium worker (22%) B: Worked in a uranium mine (10%) C: Lived in a mining camp (4%) D: Worked in a uranium mill (2%) E: Worked on a uranium mine or mill reclamation or hauled uranium ore or tailings in a pickup truck (2%) Active-mining era exposures: workers + family Many workers died from lung cancer, cohort had more family members than workers
(A) (B) (C) (D) and (E) Exposures to the environmental legacy of uranium mine and mill waste were estimated from two sources of data 1) The proximity of each resident’s home to all of the abandoned uranium mine and mill waste features (100) 2) Reported activities that increased risk of exposure to uranium mine and mill waste A: Used materials from abandoned uranium mine or mill (17%) B: Herded livestock next to uranium mine, mill or waste dump (13%) C: Drunk or contacted uranium mine waste water (13%) D: Played on a uranium tailings pile or waste dump (13%) E: Played outdoors near a uranium mine, mill, or waste dump (12%) F: Sheltered livestock in an abandoned uranium mine (2%) (F) Ongoing environmental legacy exposures
Proximity by itself consistently predicts increased disease risk 29% (374) participants live within 2 miles of AUM Only 56% of those (210) were aware they lived that close Proximity calculated from GPS measurements
Survey data were collected for 1,304 participants in face-to-face interviews Key Summary Statistics Family history of each disease also included
Various methods were applied to data analysis • Bayesian model averaging (BMA) • Logistic regression analysis • Two multivariate modeling techniques • Different models all lead to similar results and conclusions
Conditionally specified logistic regression model: Bayesian model averaging results • Bayesian “prior” values (1st column) • Tested risk factors() • Accepted risk factors () • High “Posterior” probabilities () for parameter inclusion (2nd column) • Parameter estimates (3rd column) • Conclusions based upon 128 models under consideration • Active-mining related exposure surrogate (M)relates to an odds ratio of 1.5 • Environmental legacy exposure surrogate (L)can be visualized as risk maps Note: autoimmune disease not modeled in CSLR
Mean reflects the increase in risk for each “unit” or reported exposure in the category Best (most probable) conditionally specified logistic regression model • Previous slide based on an average of 128 different, possible models • Of these, a single model was found to be the most probable -- the best fit for the data • In this model, surrogate exposure measures were significant predictors: • The active-mining related exposure surrogate (M) was associated with elevated rates of kidney disease • The environmental legacy exposure surrogate (L) was associated with elevated rates of high blood pressure
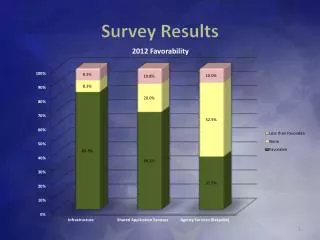
Posterior Distributions Kidney Disease (Active Mining Exposures) High Blood Pressure (Environmental Legacy Exposure) Alternate modeling approaches lead to similar conclusions • There are several ways to build a multivariate binary statistical model • Different methods of analysis lead to slightly different results • The importance of surrogate measures for exposure to uranium mine and mill waste is confirmed by various modeling approaches
1 Exposure Reported 2 Exposures Reported Maps show the impact of environmental legacy exposures and proximity • The environmental legacy surrogate for ongoing exposures predicts increased levels of high blood pressure • All other risks being equal, risk for high blood pressure increases with • proximity to abandoned uranium mine and mill waste, and • number of exposure-related activities reported
2 Exposures Reported 1 Exposure Reported Environmental legacy exposures are strong predictors of autoimmune disease risk • Best model for autoimmune disease includes 1) age and 2) surrogate measure for environmental legacy exposure • Disease risk increases with • proximity to abandoned uranium mine and mill waste, and • number of exposure-related activities reported
Summary of DiNEH Modeling Results • Basis for statistical models: • Kidney disease, diabetes, hypertension, autoimmune disease • Accepted risk factors (family history of disease, age, gender, obesity) • Locations of abandoned uranium mine and mill waste relative to homes of survey participants • Surrogate measures were developed to measure exposure: • Active mining-related exposures associated with elevated rates of kidney disease • Environmental legacy exposures associated with elevated rates of hypertension and autoimmune disease • Different statistical modeling methods (models with different mathematical structures) lead to similar results and conclusions
DiNEH Project Partners • Researchers: UNM Community Environmental Health Program and Southwest Research and Information Center • Chapters: Baca-Prewitt, Becenti, Casamero Lake, Church Rock, Coyote Canyon, Crownpoint, Iyanbito, Lake Valley, Littlewater, Mariano Lake, Nahodishgish, Ojo Encino, Pinedale, Pueblo Pintado, Smith Lake, Standing Rock, Thoreau, Torreon, White Rock, Whitehorse Lake Community • Advisory Board: Thomas Manning, Herbert Enrico, Lynnea Smith, Ed Carlisle, Jay DeGroat • Additional Support: NNEPA; NNDOH; USEPA Region 9; USACE; University of TX, Houston (Dr. Don Molony); many individuals and agencies For more information: UNM/CEHP: Toll free1-877-545-6775 SRIC: 505-262-1862 www.sric.org sric.chris@earthlink.net
NIEHS, EPA and UNM for financial support Community Advisory Board Ed Carlisle, Jay DeGroat, Herbert Enrico, Thomas Manning,Sr., Lynnea Smith, Jean Whitehorse, UNM-HSC Community Environmental Health Program & Clinical and Translational Science Center Johnnye L. Lewis, PhD; Miranda Cajero, BCH; Matthew Campen, PhD; Jeremy DeGroat; Mallery Downs, RN; Eszter Erdei, PhD; Molly Harmon; Gabriel Huerta, PhD; Curtis Miller; Bernadette Pacheco; Glenn Stark; Mary Woodruff; research nursing support Crownpoint Service Unit, I H S Virgil Davis Navajo Area IHS Lisa Allee, CNM; John Hubbard; Ryan Johnson, MD; Doug Peter, MD UT-Houston Nephrology Donald Molony, MD Southwest Research Information Center Chris Shuey, MPH, Sarah Henio-Adeky, Teddy Nez, Sandy Ramone Students Jamie deLemos, PhD – Tufts Univ. Christine George – Stanford Univ. Tommy Rock, MA, UNM Health Policy Student Christine Samuel-Nakamura, PhD Candidate, UCLA Dartmouth Ben Bostick, PhD University of Arizona Cancer Center & Northern Arizona University, NACRP Jani Ingram, PhD, Margaret Briehl, PhD USEPA Region IX Harry Allen, Rich Bauer, Clancy Tenley State of New Mexico Diagnostic Laboratory Navajo Nation EPA Air Quality Division, Public Water Supply Supervision Program, Superfund Program Navajo Nation Division of Health Former Contributors: Bess Seschillie, Bernice Norton, Jerry Elwood, Harrison Gorman, Harris Arthur (in memoriam), Alta McCabe, Margaret Menache, PhD, Alexis Kaminsky, PhD; Eastern Navajo Health Board Thanks to the many others who’ve contributed DiNEH Acknowledgements