IV fluid therapy
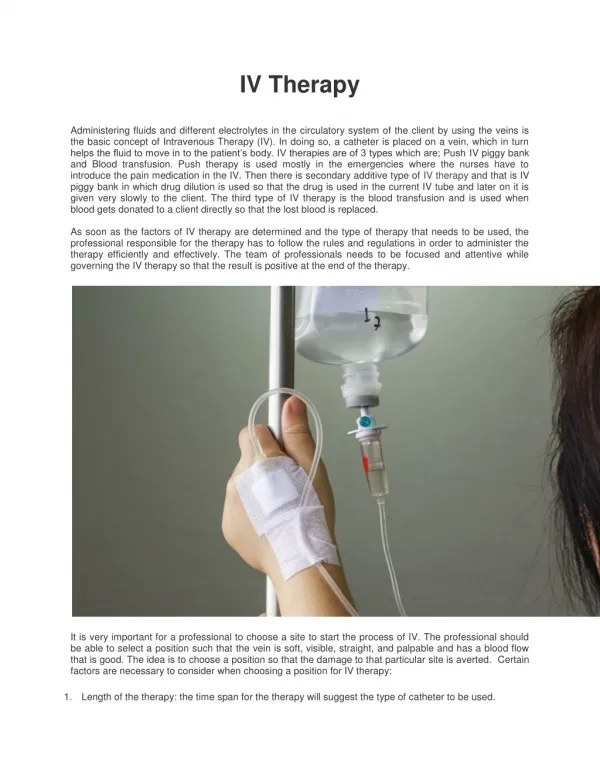
Applied Sciences Lecture Course. IV fluid therapy. Dr Cathy Armstrong SpR In Anaesthesia & Clinical Fellow in Undergraduate Medical Education Manchester Royal Infirmary April 2011. Review relevant physiology IV fluid preparations Clinical Assessment of fluid balance IV fluid strategies


IV fluid therapy
E N D
Presentation Transcript
Applied Sciences Lecture Course IV fluid therapy Dr Cathy Armstrong SpR In Anaesthesia & Clinical Fellow in Undergraduate Medical Education Manchester Royal Infirmary April 2011
Review relevant physiology IV fluid preparations Clinical Assessment of fluid balance IV fluid strategies Special circumstances Practice scenarios Objectives
Body Fluid Compartments • Total Body water is: • 60% of total body weight in males • 55% of total body weight in females
Body Fluid Compartments • 70Kg Man Solids (40%) ⅓ Interstitial fluid 11 Litres Water (60%) 42 Litres ECF 14 Litres Plasma 3 Litres ⅔ ICF 28 Litres
Insensible losses 1000ml Daily Input Vs Output
3rd space losses • 1st Spacing: Normal distribution within ECF and ICF • 2nd spacing: accumulation within the interstitial compartments: oedema formation but available for physiological exchange between compartments • 3rd spacing: Accumulation in parts of the body where it’s not available for exchange between the different compartments: Ascitis, tissue inflammation, oedema from burns/surgery
IV fluid types • Crystalloids • Colloids • Synthetic • Human
Crystalloid • “A substance in solution that can diffuse through a semipermeable membrane” • Electrolyte-containing solutions that are formulated to match to a greater or lesser extent the biochemical & osmotic features of the plasma • They do not contain high molecular weight compounds
Crystalloids • Examples • 0.9% Saline (Normal saline) • Hartmann’s (compound sodium lactate) • Glucose containing solutions • 5% Glucose • 10% Glucose • Dex-saline • 4% glucose & 0.18% saline • 5% glucose & 0.45% saline
Colloids • Solutions that contain high molecular weight proteins as well as electrolytes • Unable to diffuse through normal capillary membranes
Colloids • Examples • Gelatin-based • Gelofusine • Haemaccel • Hydroxyethyl starches (HES) • Pentastarch • 5% - Hemohes • 10% - HAES-steril • Tetrastarch - 6% (HES) • Voluven • Volulyte • Dextran 70 • Rescuflow • Human albumin solutions • HAS 5% • HAS 20% Max 1.5l / 24hr Max 2.5l / 24hr 50ml/kg/24hr (3.5l) Use in trauma, (Max 1l) 250ml followed by isotonic fluids Severe allergic reactions, coagulation effects
Distribution of IV fluids Colloid 5% Dextrose 0.9% Saline
Balanced vs unbalanced solutions • Large volumes of 0.9% saline based products have been shown to cause hyperchloraemic acidosis • Balanced solutions e.g Hartmanns, volulyte are now becoming more popular
Basis of IV fluid therapy • Does my patient need IV fluid therapy? • Why does my patient need IV fluid therapy? • Maintenance • To supply daily needs • Replacement • To replace on-going losses • Resuscitation • To correct an intravascular or extracellular deficit
Definitions • Dehydration • the loss of water and salts essential for normal body function. • Hypovolaemia • Decreased circulating plasma volume • Shock • Systemic hypoperfusion & tissue hypoxia
Types of shock • Hypovolaemic • Cardiogenic • Septic (distributive) • Obstructive
Causes of dehydration / hypovolaemia • Increased loss • Pyrexia • Vomiting • Diarrhoea • 3rd space loses – peritonitis / ascites / sepsis • Diuretics • Metabolic derangements e.g diabetes mellitus • Diabetes insipidus • Blood loss • Reduced intake
Patient observations • General ward • HR • BP • Temp • RR • Urine output (oliguria = <0.5ml/kg/hr (30ml/hr) • Critical care • IABP • CVP • CO monitoring
Basis of IV fluid therapy • Does my patient need IV fluid therapy? • Why does my patient need IV fluid therapy? • Maintenance • To supply daily needs • Replacement • To replace on-going losses • Resuscitation • To correct an intravascular or extracellular deficit
Maintenance Daily Requirement for 70kg man Fluid 2-3L Sodium – 70 – 105 mmol Potassium – 56 – 70 mmol
Maintenance regimens • Traditional approach • 1 “salt” + 2 “sweet” • Potassium replacement guided by plasma levels but if normal - replace with daily requirements (60mmol)
Exercise 1 • Tom Jones - 70Kg man, NBM, No extra losses • Hospital number M10/5678 • DOB 12/12/1962 • Ward 12 • Serum potassium 3.8mmol/l Prescribe maintenance fluids for the next 24 hrs 1 x 1000mls 0.9% saline with 20mmol potassium chloride 2 x 1000mls 5 % dextrose with 20mmol potassium chloride
Replacement fluids • Maintenance plus replacement of on-going losses • Consider the type of loss & it’s likely electrolyte content
Resuscitation • Treating deficit of intravascular or extracellular volume • Caution • Renal impairment • “pump failure” – reduced LV function
Exercise 2 • Tom Jones – • Hospital number M10/5678 • DOB 12/12/1962 • Ward 12 Day 3 Post-op laparotomy & ileostomy – minimal output from ileostomy HR – 118 BP –85/60 RR 22 T 38.50C Urine output 10mls/hr Currently has 1000mls 5%Glucose with 20mmol KCL running over 8hrs Prescribe appropriate fluids for the immediate period Fluid bags available in store cupboard: 1000mls 0.9% Saline 1000mls 5% Glucose 1000mls Hartmanns 1000mls 0.9% saline with 20mmol KCL 1000ml 5% dextrose with 20mmol KCL 500ml Gelofusine
Crystalloids vs colloids • Controversial • Crystalloids require more volume • 5L crystalloid replaces 1L intravascular loss • Colloids • Higher incidence of allergic reactions • Compounds persist in the body • Solutions containing 0.9% saline – risk of hyperchloraemic acidosis in large volumes
Resuscitation • Do not use dextrose containing solutions • Take care with potassium containing solutions
Guidelines www.bapen.org.uk/pdfs/bapen_pubs/giftasup.pdf Forthcoming NICE guidelines – IV fluids in Hospitalised patients
Special circumstances - Paediatrics • Maintenance fluids (4,2,1 rule) • 4ml/kg/hr for 1st 10kg • 2ml/kg/hr for 2nd 10kg • 1ml/kg/hr for remaining weight • E.g 24kg child • (4x10) + (2x10) + (1x4) = 64ml/hr • Dehydration (maintenance + estimated deficit) • %dehydration x wt x 10 • E.g above child with 5% dehydration • 5 x 24 x 10 = 1200ml – to replace over 24hrs 1200/24 = 50mls/hr • Therefore Maintenance + deficit = 64+50 = 104mls/hr
Special circumstances - Burns • Parklands formula • 4ml/kg x % burned body surface area • ½ volume given over 1st 8 hours • ½ volume given over subsequent 16 hours • E.g 70kg man with 25% burns • (4x70) x 25 = 7000ml • (7000/2) / 8 = 438mls/hr (for 1st 8 hrs) • (7000/2) / 16 = 218 mls/hr (for subsequent 16 hrs)
Exams • Popular OSCE station in Year 5 • Involves choice of fluid & prescribing • Often twinned with practical skill • I:e changing bag (remember to do appropriate checks incl exp date) • Calculating & setting drip rate – most giving sets 20 drops = 1ml
Calculating drip rate • Most giving sets – 20 drops = 1ml Volume (mls) STEP 1 STEP 2 As 20÷60 = ⅓ STEP 2 & STEP3 can be combined mls/hr x ⅓ = drops/min mls/hr mls/min = = mls/hr Time (hrs) 60 Mls/min x 20 = drops per min STEP 3
Exercise - Calculating drip rate • 1000mls over 8 hours 1000 (mls) STEP 1 STEP 2 As 20÷60 = ⅓ STEP 2 & STEP3 can be combined mls/hr x ⅓ = drops/min 125mls/hr 2 mls/min = = 125mls/hr 8 (hrs) 60 2 mls/min x 20 = 40 drops per min STEP 3