Download
1 / 1
10 likes | 124 Vues
Q Fever Endocarditis: An Unusual Presentation Martin Espinosa Ginic¹, MD, Allen T. Griffin,² MD, and Raul Nakamatsu,² ,3 MD Department of Medicine, Division of Cardiovascular Medicine¹ and Division of Infectious Diseases², Robley Rex VAMC 3. ABSTRACT. B. DISCUSSION. A.

E N D
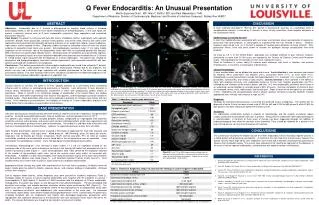
Q Fever Endocarditis: An Unusual Presentation Martin Espinosa Ginic¹, MD, Allen T. Griffin,² MD, and Raul Nakamatsu,²,3 MD Department of Medicine, Division of Cardiovascular Medicine¹ and Division of Infectious Diseases², Robley Rex VAMC3 ABSTRACT B DISCUSSION A Q fever, originally described in 1937 by E.H. Derrick in Queensland, Australia, as a pathologic entity in slaughterhouse workers, is caused by C. burnetii, a small, strictly intracellular, Gram-negative bacterium of the Coxiellaceae family. Epidemiology of Coxiella burnetii: Q fever has traditionally been associated with rural areas and livestock where aerosolization of organisms, particularly from birth products, or consumption of unpasteurized milk has resulted in illness. However, exposure need not be rural, as C. burnetii is capable of traveling great distances to cause infection. Pets, particularly felines, have also been shown to transmit the pathogen through aerosolization from birth products. As many as 2.9 % of the United States population has serologic evidence of past infection; however, consistently no more than 20-160 cases are reported to the Centers for Disease Control and Prevention yearly. The preponderance of instances are from rural, midwestern states. Given its hardiness in nature, ability to traverse great distances and result in infection, and extreme infectiousness, C. burnetti is a feared agent of bioterrorism. Clinical Presentation: Q fever manifestations can be divided into acute and chronic. Acute infection is more common and marked by hepatitis (40%), pneumonia and hepatitis (20%), pneumonia alone (17%), or fever alone (17%). Exceptionally unusual presentations include meningoencephalitis (1%), meningitis (1%), myocarditis (0.7%), pericarditis, osteomyelitis, and uveitis or optic neuritis. Chronic infection is more common in the elderly or those with impaired immunity, with endocarditis being by far the most frequent presentation (60-70%), followed by rare infections of the arteries, bones, and liver. In Q fever endocarditis, prosthetic heart valves or an underlying valvular disorder is invariably present (88% of cases). Common complaints of chronic Q fever are headache, fevers, chills, night sweats, and muscle pain. Signs of heart failure are typical as are embolic events. Vegetations are characteristically small or absent; abscess formation is scarcely reported. Despite appropriate care, mortality rates may be as high as 24%. Diagnosis: Serology, by microimmunofluorescence, is currently the preferred means of diagnosis. The optimal titer for diagnosis of acute Q fever has been shown to be ≥1:200 for IgG and ≥1:50 for IgM (phase II) while ≥1:800 for IgG (phase I) has been found to be optimal for chronic Q fever. Treatment: For endocarditis, combination therapy is superior to monotherapy, and the majority of patients require surgery, particularly if paravalvular extension is present. Doxycycline in combination with hydroxychloroquine is recommended. A minimum of three years of therapy has been suggested although the addition of hydroxychloroquine may allow the duration to be shortened. Titers should be followed for a period of five years to help ensure no recurrence transpires off treatment. Objectives: Endocarditis due to C. burnetii is distinguished by negative blood cultures in standard bacteriologic media as well as small or even absent vegetations on echocardiography. In this case report, we present a distinctly unusual case of Q fever endocarditis marked by large vegetations and associated paravalvular abscess. Case Report:The patient is a 50-year-old male with history of diabetes mellitus, nephropathy with nephrotic syndrome, diastolic heart dysfunction, coronary artery disease, and severe aortic stenosis with aortic valve replacement who presented with gradually worsening shortness of air, weight loss, fatigue, severe headaches, night sweats, and an episode of fever. Diagnostic studies revealed no immediate source of fever, but clinical evidence of congestive heart failure was present. Echocardiography revealed a large 1.7 cm highly mobile vegetation on the ventricular side of the bioprosthetic aortic valve with an associated paravalvular abscess. MRI of the brain revealed multiple embolic lesions. All blood cultures off antibiotics were persistently negative. Serologies for potential causes of culture-negative endocarditis were procured and revealed titers of C. burnetii of 1:2048 (phase I IgG) consistent with the diagnosis of Q fever endocarditis. The patient was initiated on doxycycline and hydroxychloroquine, had aortic valvular replacement, and recovered uneventfully with later decline associated with medication non-compliance. Conclusions: This patient presented with culture-negative endocarditis later found to be related to C. burnetii, the agent of Q fever. Quite distinct from most cases of endovascular infection due to this organism, this patient not only had a distinctly large vegetation with embolic phenomenon to the brain, but also had paravalvular spread. This case illustrates that Q fever should be considered in the differential diagnosis of all cases of culture negative endocarditis regardless of vegetation size. RV RV LV LV LA LA C D LV RV AV RA LA INTRODUCTION Coxiella burnetii (C. burnetii), the agent of Q fever, typically presents as a self-limiting illness resembling influenza with or without an accompanying pneumonia or hepatitis. Less commonly, Q fever becomes a chronic illness manifested by endovascular involvement in those with predisposing cardiac lesions or prostheses. While C. burnetii is an uncommon etiology of endocarditis in the United States, the cardiac valvular lesions often differ fundamentally from those of most bacteria, and the pathogen cannot be isolated in standard media. These distinctions offer clues to the pathogen’s presence for clinicians less familiar with this illness. In the following case presentation, we elucidate an instance of Q fever endocarditis acquired in the United States that is marked by unusual cardiac manifestations. Figure 1. Echocardiography: A) Trasthoracic parasternal long axis view during isovolumetric contraction revealing large vegetation extending to the anterior leaflet of the mitral valve. B) Trasthoracic parasternal long axis view during end systole with partial occlusion of the left ventricular outflow tract by large vegetation. C) Apical four chamber view with vegetation attached at the junction of aortic valve ring to base of anterior mitral valve. D) Transeshophageal short axis view at the aortic valve level revealing periprosthetic aortic rood abscess. RV: Right ventricle, LV: Left ventricle, RA: Right atrium, LA: Left atrium, AV: Aortic Valve. CASE PRESENTATION A 50-year-old Caucasian male presented with three weeks of shortness of breath, headaches, and generalized swelling. He noted associated night sweats, malaise, weight loss, and one episode of fever to 101°F. The patient’s past medical history included diabetes mellitus complicated by nephropathy with nephrotic syndrome, coronary artery disease, and severe aortic stenosis with bioprosthetic aortic valve replacement and coronary artery bypass grafting one year prior to presentation. He resided in a suburban area of Kentucky and had never traveled outside the United States. However, he reported working on a dairy farm until 2002. Upon hospital presentation, physical exam revealed a chronically ill appearing thin male with anasarca and signs of muscle wasting. Vital signs were: blood pressure, 188/104mmHg; pulse, 80 beats per minute; respiratory rate, 22 breaths per minute; temperature, 96.2F; and O2 saturation, 97% on room air. Cardiac auscultation revealed a loud midsystolic murmur heard best in the left parasternal area on expiration. Lung auscultation revealed bibasilar crackles. Chest roentgenogram showed mild pulmonary edema. Transthoracic echocardiogram (TTE) revealed a highly mobile 1.7 x 0.9 cm vegetation located on the ventricular side of the aortic valve extending to the base of the anterior MV leaflet that protruded into the LV outflow tract during systole (Figure 1). Later, transesophageal echo (TEE) confirmed the vegetation attached at the junction of the prosthetic aortic valve ring to the anterior mitral valve leaflet, all consistent with endocarditis. In addition, a 0.5cm thick echogenic layer along the posterior aspect of the aortic root consistent with paravalvular abscess was noted (Figure 1). Left Ventricular Ejection Fraction (LVEF) was 51%. ECG showed normal sinus rhythm with no signs of acute ischemia or conduction abnormalities. Appropriate diuretic therapy was given with improvement of the heart failure symptoms. Antibiotics were not begun initially given the patient’s stability, subacute course, and unknown etiology of endocarditis. All blood cultures were negative. Due to negative blood cultures, further diagnostic tests were pursued for fastidious organisms (Table 2). Serologic studies for causes of culture-negative endocarditis were negative with the exception of a phase I immunoglobulin G (IgG) against C. burnetii at 1:2048 consistent with the diagnosis of Q fever endocarditis. Subsequently, the patient was begun on oral doxycycline and hydroxychloroquine. He later developed mild dysarthria and vertigo, and embolic posterior circulation strokes where confirmed by MRI (Figure 2). The patient was taken to cardiac surgery emergently where he had replacement of his bioprosthetic aortic valve with a mechanical prosthesis, and debridement with reconstruction of the aortic root. He recovered uneventfully; repeat phase I titers before hospital discharged declined to 1:1024. Unfortunately, the patient was erratically compliant with his medications and months later developed progressive paravalvular aortic regurgitation with significant dehiscence of the prosthetic valve and consequent heart failure that led to his death. The valvular dehiscence was thought to be related to recurrence of infection. CONCLUSIONS The current case illustrates the indolent course of Q fever endocarditis with its invariably negative cultures in a feeble patient with preexisting valvulopathy. In contrast to the vast majority of Q fever cases, however, the patient not only had a large aortic valve vegetation, but he also had a distinctly uncharacteristic paravalvular abscess that mandated surgery. The current case emphasizes the need to be cognizant of the diagnosis in all cases of culture-negative endocarditis, including those with atypical cardiac manifestations. Figure 2: Axial T2-Flair MRI image revealing multiple areas of abnormally restricted diffusion in the posterior circulation territory, largest in the left cerebellar hemisphere. Findings are consistent with tromboembolic stroke lesions. REFERENCES Brouqui P, Dupont HT, Drancourt M, et al. Chronic Q fever. Ninety-two cases from France, including 27 cases without endocarditis. Arch Intern Med 1993;153:642-48. Scott JW, Baddour LM, Tleyjeh IM, et al. Q fever endocarditis: the Mayo Clinic experience. Am J Med Sci2008;336:53-7. Fournier PE, Thuny F, Richet R, et al. Comprehensive diagnostic strategy for blood culture–negative endocarditis: A prospective study of 819 new cases. Clin Infect Dis2010;51:131–40. Raoult D, Tissot-Dupont H, Foucault C, et al. Q fever 1985-1998. Clinical and epidemiologic features of 1,383 infections. Medicine (Baltimore) 2000;79:109-23. Lepidi H, Houpikian P, Liang Z, et al. Cardiac valves in patients with Q fever endocarditis: microbiological, molecular, and histologic studies. J Infect Dis2003;187:1097-1106. Fort S, Fraser AG, Fox KA. Extensive aortic valve ring abscess formation: a rare complication of Q fever endocarditis. Postgraduate Medical Journal 1989;65:384-86. Raoult D, Houpikian P, TissotDupont H, et al. Treatment of Q fever endocarditis: comparison of 2 regimens containing doxycycline and ofloxacin or hydroxychloroquine. Arch Intern Med 1999;159:167-73. Million M, Thuny F, Richet H, et al. Long-term outcome of Q fever endocarditis: a 26-year personal survey. Lancet Infect Dis2010;10:527-35.