Download
1 / 47
500 likes | 763 Vues
Living W ith Diabetes. November 21, 2013 JP Morgan Chase Michael Bergman, MD, FACP Clinical Professor of Medicine NYU School of Medicine. Epidemiology. Diabetes in the United States. Nearly 26 million people in the U.S. have diabetes 7 million people with diabetes are undiagnosed

E N D
Living With Diabetes November 21, 2013 JP Morgan Chase Michael Bergman, MD, FACP Clinical Professor of Medicine NYU School of Medicine
Diabetes in the United States • Nearly 26 million people in the U.S. have diabetes • 7 million people with diabetes are undiagnosed • 8.3% of the U.S. population • 26.9% of U.S. residents aged 65 years and older • 1.9 million Americans aged 20 years or older were newly diagnosed with diabetes in 2010 • Every 17 seconds, someone is diagnosed with diabetes Source: National Diabetes Fact Sheet, 2011
Hyperglycemia: Can Cause Serious Long-Term Problems Chronic complications of diabetes • Blindness • Kidney disease • Nerve damage • Amputation • Heart attack • Stroke
Burden of Diabetes in the United States • The leading cause of: • new blindness among adults • kidney failure • non-traumatic lower-limb amputations • Increases the risk of heart attack and stroke by 2-4 fold • 7th leading cause of death • Mortality rates 2-4 times greater than non-diabetic people of the same age • Total direct and indirect cost of diagnosed diabetes is $245 billion a year • 1 in 5 health care dollars is spent caring for someone with diagnosed diabetes Source: Centers for Disease Control and Prevention
1994 2000 1994 2000 No Data <4.5% 4.5-5.9% 6.0-7.4% 7.5-8.9% >9.0% No Data <14.0% 14.0-17.9% 18.0-21.9% 22.0-25.9% >26.0% Age-adjusted Percentage of U.S. Adults with Obesity or Diagnosed Diabetes Obesity (BMI ≥30 kg/m2) 2009 OBESIT Y Diabetes DIABETES 2009 CDC’s Division of Diabetes Translation. National Diabetes Surveillance System available at http://www.cdc.gov/diabetes/statistics
The Diabetes Epidemic: Global Projections, 2010–2030 IDF. Diabetes Atlas 5th Ed. 2011
How did this happen? Presentation Title Goes Here
Pre-diabetes Presentation Title Goes Here
What is Pre-diabetes? • A serious health condition that increases the risk of developing type 2 diabetes, heart disease and stroke • Blood glucose levels are higher than normal but not yet diabetes • Impaired Fasting Glucose (IFG) • Impaired Glucose Tolerance (IGT): non-fasting • Combination (IFG+IGT) = highest risk for progression to diabetes • 1 in 3 American adults (79 million) have prediabetes • Occurs before type 2 diabetes • Most people with prediabetes don’t know they have it
Who Is Likely To Have Pre-diabetes? • 45 years of age or older • Overweight • Have a parent with diabetes • Have a sister or brother with diabetes • Family background is African American, Hispanic/Latino, American Indian, Asian American or Pacific Islander. • Developed diabetes while pregnant (gestational diabetes), or gave birth to a baby weight 9 pounds or more • Physically active less than 3 times a week
Pre-diabetes • In US, estimated lifetime risk of acquiring diabetes is 32.8% for males and 38.5% for females • 35% of adults> 20 years have Pre-diabetes • 50% of adults > 65 years have Pre-diabetes • 7% are aware of condition • 1/3 of individuals with IFG or IGT and 2/3 with both will develop diabetes within 6 years • Annual risk of progression is 5-10% • Long preclinical phase presents window of opportunity to intervene to prevent progression
350 300 250 200 150 IFGIGT DM Relative to normal 100 Insulin resistance 250 200 (%) 150 100 At risk for diabetes Insulin level Beta-cell dysfunction 50 0 Atherosclerosis Cardiovascular event Natural History Metabolic Syndrome Glucose Post-prandial glucose mg/dL Fasting glucose 25 30 0 5 10 15 20 -10 -5 Years Kendall, International Diabetes Center
Diabetes Presentation Title Goes Here
Types of Diabetes • Two Main Types: • Type 1: • Pancreas makes too little or no insulin • Type 2: • Cells do not use insulin well (insulin resistance) • Ability for pancreas to make insulin decreases over time • Gestational • Other Types
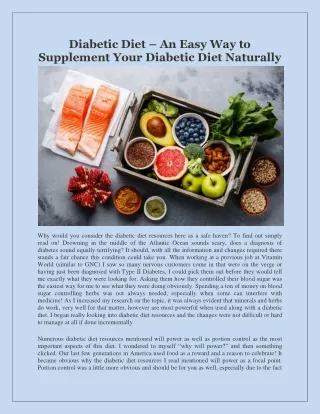
What Happens When We Eat? After eating, most food is turned into glucose, the body’s main source of energy.
HighBlood Glucose (Hyperglycemia) Normal Blood Glucose Control In people without diabetes, glucose stays in a healthy range because: In diabetes, blood glucose builds up for several possible reasons… • Insulin is released at the right times and in the right amounts Liver releases too much glucose Too little insulin is made Insulin helps glucose enter cells Cells can’t use insulin well
Type 1 Diabetes Type 1 Diabetes • 1 in 20 people with diabetes have Type 1 • Most people are under age 20 when diagnosed • Body can no longer make insulin • Insulin is always needed for treatment Previously called insulin-dependent or juvenile onset diabetes. Develops when the body’s immune system destroys pancreatic beta cells, the only cells in the body that make the hormone insulin, which regulated blood glucose. To survive, people with Type 1 diabetes must have insulin delivered by injection or a pump. Type 1 usually strikes children and young adults, although disease onset can occur at any age. In adults, Type 1 diabetes accounts for approximately 5% of all diagnosed cases of diabetes. Risk factors may be autoimmune, genetic, or environmental. No known way to prevent Type 1 Diabetes
Before and After Insulin Treatment Discovery of insulin in 1921 changed type 1 from a death sentence to a chronic disease 7-year-old child before and 3 months after insulin therapy
Symptoms of Type 1 Diabetes Symptoms usually start suddenly • Weight loss • Loss of energy • Increased thirst • Frequent urination • Diabetic ketoacidosis (emergency condition of nausea, vomiting, dehydration. Can lead to coma)
Managing Type 1 Diabetes • Blood glucose monitoring • Education • Healthy food choices • Physical activity • Insulin
Type 2 Diabetes • Previously called non-insulin dependent diabetes mellitus or adult-onset diabetes. • Accounts for about 90-95% of all diagnosed cases of diabetes. • Usually begins as insulin resistance, when the cells do no use insulin properly. • As need for insulin increases, the pancreas gradually loses its ability to produce it. • Type 2 is associated with older age, obesity, family history of diabetes, history of gestational diabetes, impaired glucose metabolism, physical inactivity and race/ethnicity. • Most people with diabetes have type 2 • Most people are over age 40 when diagnosed, but type 2 is becoming more common younger adults, children and teens
Risk Factors for Type 2 Diabetes • Being overweight • Sedentary lifestyle • Family history of Type 2 diabetes • History of gestational diabetes • Older Age • Ethnic/racial background: • African American • Hispanic/Latino • Native American • Asian American
Symptoms of Type 2 Diabetes • Usually subtle or no symptoms in early stages: • Increased thirst • Increased urination • Feeling tired • Blurred vision • More frequent infections • Symptoms may be mistaken for other situations or problems • 1 in 4 with type 2 aren’t aware they have it
Treatmentfor Type 2: Diabetes May Change Over a Lifetime Always Includes: • Education • Healthy eating • Blood glucose monitoring • Physical Activity May Include: • Medications, including insulin
Other Types of Diabetes Gestational Diabetes • Form of glucose intolerance diagnosed in pregnancy • Occurs more frequently among African Americans, Hispanic/Latino Americans, and American Indians • More common among obese women and women with a family history of diabetes. • During pregnancy, gestational diabetes requires treatment to optimize maternal blood glucose levels to reduce risk of complications to the infant. Other Types Result from: • Specific genetic conditions • Surgery • Medications • Infections • Pancreatic disease and other illnesses Such types account for 1 – 5% of all diagnosed cases.
Prevention Strategies Presentation Title Goes Here
Joslin, EP. The Prevention of Diabetes Mellitus [JAMA 1921; 76 (2):79-84] “There are entirely too many diabetic patients in the country. Statistics for the last thirty years show so great an increase in the number that, unless this were in part explained by a better recognition of the disease, the outlook for the future would be startling.” ”The physician should take pride in the prevention of diabetes in his practice. Obese patients should be frankly told that they are candidates for diabetes.” ”But it is to the diabetic patient and his relatives that one can look most confidently for help in preventing diabetes. They should be encouraged to disseminate information about its prevention.”
Preventive Efforts Are Key • Most of the diabetes costs are due to end-stage complications • Investment of resources into early diagnosis, patient education, prevention and treatments pays off in: • Longer lives • Increased productivity • Reduced costs over the long term
Is There Any Good News? • Yes!! We can reduce the chances of developing type 2 diabetes in high-risk people (weight loss, exercise, medications) • Yes!! We canreduce the chances of developing diabetes complications through: • Blood glucose control (diet, monitoring, medication) • Blood pressure control • Cholesterol control • Regular visits to healthcare providers • Early detection and treatment of complications
Steps to Lower Your Risk of Diabetes Complications • A1C < 7 • Blood pressure < 140/80 • Cholesterol (LDL) < 100, statin therapy for high risk • Get help to quit smoking • Be active • Make healthy food choices • Take care of your feet • Get recommended screenings and early treatment for complications
Personal Road to Prevention • Know your Fasting Glucose Level • 100-125 mg/dl: prediabetes (IFG) • ~ 90-100 mg/dl, regular follow-up if: • Overweight/obese • Triglyceride levels elevated • Presence of other risk factors (e.g., family history, gestational diabetes) • Gestational Diabetes: 35-60% over 10-20 years • Know your Non-Fasting Glucose Level • Oral Glucose Tolerance Test (OGTT): • 2-hour level =140-199 mg/dl (IGT)
Personal Road to Prevention • Know your Hemoglobin A1c level: • Levels = 5.7-6.0% suggest moderate risk for progression to diabetes • Levels = 6.1-6.4% suggest high risk for progression to diabetes • Level > 6.5% diagnostic of diabetes • Know your blood pressure • Know your cholesterol level
Diabetes:10 Myths and Facts Presentation Title Goes Here
Myth 1: Diabetes is not that serious of a disease. Fact:If you manage your diabetes properly, you can prevent or delay diabetes complications. However, diabetes causes more deaths a year than breast cancer and AIDS combined. Two out of three people with diabetes die from heart disease or stroke. Myth 2: If you are overweight or obese, you will eventually develop type 2 diabetes. Fact:Being overweight is a risk factor for developing this disease, but other risk factors such as family history, ethnicity and age also play a role. Unfortunately, too many people disregard the other risk factors for diabetes and think that weight is the only risk factor for type 2 diabetes. Most overweight people never develop type 2 diabetes, and many people with type 2 diabetes are at a normal weight or only moderately overweight.
Myth 3: Eating too much sugar causes diabetes. • Fact:The answer is not so simple. Type 1 diabetes is caused by genetics and unknown factors that trigger the onset of the disease; type 2 diabetes is caused by genetics and lifestyle factors. Being overweight does increase your risk for developing type 2 diabetes, and a diet high in calories from any source contributes to weight gain. Research has shown that drinking sugary drinks is linked to type 2 diabetes. • The American Diabetes Association recommends that people should limit their intake of sugar-sweetened beverages to help prevent diabetes. Sugar-sweetened beverages include beverages like: • regular soda • fruit punch • fruit drinks • energy drinks • sports drinks • sweet tea • other sugary drinks. • These will raise blood glucose and can provide several hundred calories in just one serving! • See for yourself: Just one 12-ounce can of regular soda has about 150 calories and 40 grams of carbohydrate. This is the same amount of carbohydrate in 10 teaspoons of sugar! • One cup of fruit punch and other sugary fruit drinks have about 100 calories (or more) and 30 grams of carbohydrate.
Myth 4: People with diabetes should eat special diabetic foods. Fact:A healthy meal plan for people with diabetes is generally the same as a healthy diet for anyone – low in fat (especially saturated and trans fat), moderate in salt and sugar, with meals based on whole grain foods, vegetables and fruit. Diabetic and "dietetic" foods generally offer no special benefit. Most of them still raise blood glucose levels, are usually more expensive and can also have a laxative effect if they contain sugar alcohols. Myth: If you have diabetes, you should only eat small amounts of starchy foods, such as bread, potatoes and pasta. Fact 5:Starchy foods can be part of a healthy meal plan, but portion size is key. Whole grain breads, cereals, pasta, rice and starchy vegetables like potatoes, yams, peas and corn can be included in your meals and snacks. Wondering how much carbohydrate you can have? A place to start is about 45-60 grams of carbohydrate per meal, or 3-4 servings of carbohydrate-containing foods. However, you may need more or less carbohydrate at meals depending on how you manage your diabetes. You and your health care team can figure out the right amount for you. Once you know how much carb to eat at a meal, choose your food and the portion size to match.
Myth 6: People with diabetes can't eat sweets or chocolate. Fact:If eaten as part of a healthy meal plan, or combined with exercise, sweets and desserts can be eaten by people with diabetes. They are no more "off limits" to people with diabetes than they are to people without diabetes. The key to sweets is to have a very small portion and save them for special occasions so you focus your meal on more healthful foods. Myth 7: You can catch diabetes from someone else. Fact:No. Although we don’t know exactly why some people develop diabetes, we know diabetes is not contagious. It can't be caught like a cold or flu. There seems to be some genetic link in diabetes, particularly type 2 diabetes. Lifestyle factors also play a part. Myth 8: People with diabetes are more likely to get colds and other illnesses. Fact:You are no more likely to get a cold or another illness if you have diabetes. However, people with diabetes are advised to get flu shots. This is because any illness can make diabetes more difficult to control, and people with diabetes who do get the flu are more likely than others to go on to develop serious complications.
Myth 9: Fruit is a healthy food. Therefore, it is ok to eat as much of it as you wish. Fact:Fruit is a healthy food. It contains fiber and lots of vitamins and minerals. Because fruits contain carbohydrates, they need to be included in your meal plan. Talk to your dietitian about the amount, frequency and types of fruits you should eat. Myth 10: If you have type 2 diabetes and your doctor says you need to start using insulin, it means you're failing to take care of your diabetes properly. Fact:For most people, type 2 diabetes is a progressive disease. When first diagnosed, many people with type 2 diabetes can keep their blood glucose at a healthy level with oral medications. But over time, the body gradually produces less and less of its own insulin, and eventually oral medications may not be enough to keep blood glucose levels normal. Using insulin to get blood glucose levels to a healthy level is a good thing, not a bad one.