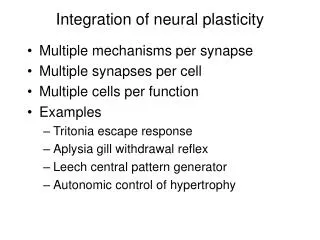
Neural Plasticity
Neural Plasticity. Ashley Maurer. What is Neural Plasticity?. Also called Neural Adaptation It is the ability of the CNS to change & adapt in response to environmental cues, experience, behavior, injury or disease

Neural Plasticity
E N D
Presentation Transcript
Neural Plasticity Ashley Maurer
What is Neural Plasticity? • Also called Neural Adaptation • It is the ability of the CNS to change & adapt in response to environmental cues, experience, behavior, injury or disease • Neurons possess the ability to alter their structure and function in response to a variety of internal & external pressures, including behavioral training • Thus, it the mechanism by which the brain encodes experience & learns new behaviors, and by which a damaged brain relearns lost behavior in response to rehabilitation
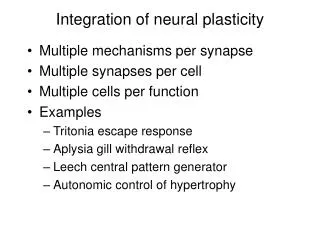
Plasticity is associated with… • Decreases, increases, and shifts in brain activation to facilitate the behavioral improvement • Reallocation in hemispheric resources • Example: relative dominance of left and right hemispheres • Recruitment of additional brain regions • Strengthening of an anatomical structure • Example: Increased white-matter density • Functional Connections • Increased coherence among regions in neural pathways • Remember Hebb told us, “Neurons that fire together, wire together.”
Principles of Neural Plasticity(Kleim & Jones, 2008; Ludlow, et al., 2008) • Principle 1: Use it or Lose it • Principle 2: Use it & Improve it • Principle 3: Specificity • Principle 4: Repetition Matters • Principle 6: Time Matters • Principle 7: Salience Matters • Principle 8: Age Matters • Principle 9: Transference • Principle 10: Interference
Principle 1: Use it or Lose it • If a neural circuit is not actively engaged in task performance for an extended period of time, it will degrade in function
Principle 2: Use it & Improve it • Training that drives a specific brain function can lead to an enhancement of both function & structure of the neural mechanisms involved in that behavior • Speech & Limb movements are different • Speech movements are learned throughout childhood, are used for several hours daily throughout a lifetime, and required precision to achieve auditory targets
Principle 3: Specificity • The nature of the training experience dictates the nature of the plasticity • Changes in neural functions may be limited to the specific function being trained • Example: Training on lip strength may benefit the generalized control for lip movement & force, but may not spontaneously transfer to speech production • Debate: Can training on non-speech oral behaviors enhance speech production • True: repetition of isolated syllables is not equivalent to speech production • However, studies show there are both commonalities & differences in the neural substrates involved in speech & non-speech behaviors
Principle 4: Repetition Matters • Induction of plasticity requires sufficient repetition • Repetition of a newly learned or relearned behavior may be required to induce lasting neural change • Therefore, the number of repetitions per session and the number of sessions required for a behavior to become consolidated needs to be established for speech and voice motor control rehabilitation
Principle 5: Intensity Matters • Induction of plasticity requires sufficient training intensity • But remember… • May not be appropriate for people with MND that are easily fatigued • Medical status & other factors should be considered before assuming that intensive training can produce behavioral changes and neural plasticity • Maladaptive responses to intense motor treatment programs may be fatigue & possible muscle damage
Principle 6: Time Matters • Different forms of neural plasticity may occur at different times in response to treatment • Therapy promoting neural restructuring should work anytime, but there may be time windows in which it is particularly effective in direction the lesion-induced reactive plasticity • Time delays may also allow for the greater establishment of self-taught compensatory behaviors, some of which may interfere with rehabilitative training efforts.
Principle 7: Salience Matters • Training experience must be sufficiently salient to induce plasticity • Neural plasticity may be enhanced when the movement is purposeful & related to the behavior being trained • Importance to speech: simple repetitive movements or strength may not enhance skilled movements & have less potential for inducing speech production for communication • Training in voice and speech may need to involve meaningful communication.
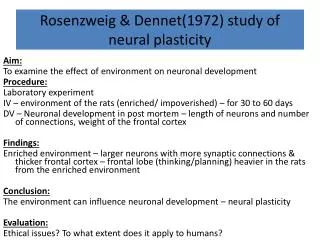
Principle 8: Age Matters • Adult brains are capable of plastic adaptation to injury including some degree of structural reorganization • Training-induced plasticity occurs more readily in younger brains • It is unknown whether learning some aspect of speech production, such a consonant articulation, may be more affected by aging than others
Principle 9: Transference • Ability of plasticity following training in one set of neural circuits may promote concurrent or subsequent plasticity • It is important to determine if a particular therapy is responsible for the enhancement of another behavior or whether transference occurs regardless of the type of therapy
Principle 10: Interference • Plasticity causing changes in neural function can also impede the induction of other behaviors or skills • Therapy that benefits one skill may interfere with performance of another • Perhaps enhancing some speech skills such as articulation might interfere with other aspects such as prosody or rate • Retained functions may interfere with the recovery of lost functions after injury.
References: Duffy, J. R. (2005). Motor speech diorders: Substrates, differential diagnosis, and management. St. Louis, MI: Elsevier Mosby. Kleim, J. A., & Jones T. A. (2008). Principles of experience-dependent neural plasticity: Implications for rehabilitation after brain damage. Journal of Speech, Language, and Hearing Research, 51, 225–239. Ludlow, C. L., Hoit, J. , Kent, R., Ramig, L. O., Shrivastav, R. Strand, E., Yorkston, K., & Sapienza, C. M. (2008). Translating principles of neural plasticity into research on speech motor control recovery and rehabilitation. Journal of Speech, Language, and Hearing Research, 51, 240–258. Zhang, Y. & Wang, Y. (2007). Neural plasticity in speech acquisition and learning. Bilingualism: Language and Cognition, 10(2) 147–160.