Download
1 / 23
270 likes | 1.21k Vues
Disorders of the Pituitary Gland. Dr. Belal M. Hijji, RN. PhD May 2 nd , 2012. Learning Outcomes. By the end of this lecture, students should be able to: Discuss the pituitary functions, dysfunction, and pathophysiology.

E N D
Disorders ofthe Pituitary Gland Dr. Belal M. Hijji, RN. PhD May 2nd, 2012
Learning Outcomes By the end of this lecture, students should be able to: • Discuss the pituitary functions, dysfunction, and pathophysiology. • Describe clinical manifestations of pituitary tumors, assessment and diagnostic findings, and an overview of medical management. • Define diabetes insipidus, describe its manifestations, diagnostic evaluation, medical and nursing management.
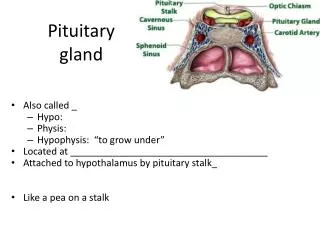
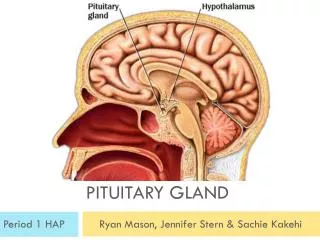
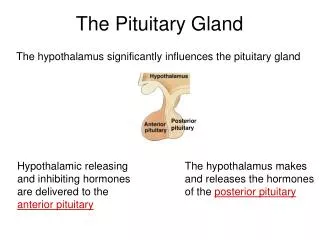
Pituitary Functions & Dysfunction • Master gland • Controlled by the hypothalamus • Has 3 lobes; anterior, posterior, and intermediate. • Anterior lobe: Synthesises & secretes GH, prolactin, ACTH, TSH, FSH, and LH, and melanocyte-stimulating hormone. • Posterior lobe: Stores & releases oxytocin and anti diuretic hormone (ADH) produced by the hypothalamus. The ADH • controls the excretion of water by the kidney; its secretion is stimulated by a decrease in blood pressure.
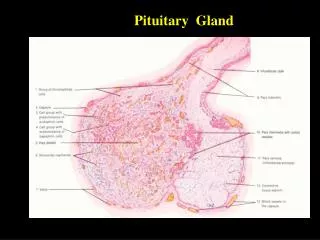
Endocrine glands in the human head and neck and their hormones 5
Pathophysiology • Abnormalities of the pituitary gland result from: • Oversecretion or; • Undersecretion • Abnormalities of posterior and anterior lobes can occur independently. • Oversecretion most commonly involves ACTH leading to Cushing’s syndrome, or GH leading to acromegaly. • Undersecretion: Involves the anterior pituitary hormones. • Deficient production of the ADH → diabetes insipidus, which is the most common disorder of the posterior lobe in which abnormally large volumes of dilute urine are excreted.
Hypopituitarism • It is hypofunction of the pituitary gland. • It results from disease of the pituitary gland itself (destruction of the anterior lobe) or of the hypothalamus. • Panhypopituitarism is total absence of all pituitary secretions and is rare. Postpartum pituitary necrosis is more likely to occur in women with severe blood loss, hypovolemia, and hypotension at the time of delivery. • Is a complication of radiation therapy. The total destruction of the pituitary gland results in extreme weight loss, emaciation, atrophy of all endocrine glands and organs, hair loss, impotence, amenorrhea, hypometabolism, and hypoglycemia. Coma and death may occur.
Pituitary Tumors • Are usually benign. • Their location and effects on hormone production can be life threatening.
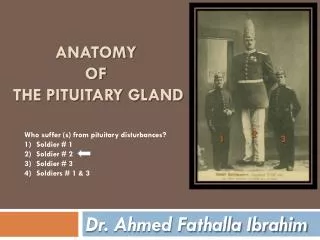
Clinical Manifestations Associated with Pituitary Tumors • Gigantism (slide 13). The affected person is • > 7 feet tall and large in all proportions • so weak that s(h)e can hardly stand • Excessive skeletal growth occurs only in the feet, the hands, the molar eminences, the nose, and the chin, giving rise to acromegaly.
Cushing’s syndrome. Features include: • Masculinization & amenorrhea in women, truncal obesity, hypertension, osteoporosis, and polycythemia. • Patients are often obese and somnolent [feeling sleepy]. • Exhibit fine, scanty [inadequate] hair, dry, soft skin. • Experience headaches, loss of libido, and visual defects progressing to blindness. Other signs and symptoms include polyuria, polyphagia, and a subnormal body temperature.
Assessment and Diagnostic Findings • Careful history and physical examination. • Assessment of visual acuity and visual fields. • Computed tomography (CT) and magnetic resonance imaging (MRI). • Serum levels of pituitary hormones. • Serum levels of hormones of target organs (eg, thyroid, adrenal).
Medical Management • Radiation therapy. • Surgical removal of the pituitary gland. • It is the treatment of choice in patients with Cushing’s syndrome due to excessive production of ACTH by a tumor of the pituitary gland. • Hypophysectomy may also be performed as a palliative measure to relieve bone pain secondary to metastasis of malignant lesions of the breast and prostate.
Diabetes Insipidus • Diabetes insipidus is a disorder of the posterior lobe of the pituitary gland. • ADH is deficient. • Causes could be head trauma, brain tumor, or irradiation of the pituitary gland, infections of the CNS (meningitis, encephalitis, tuberculosis) or tumors (eg, metastatic disease, lymphoma of the breast or lung). Another cause is failure of the renal tubules to respond to ADH; this may be related to hypokalemia,hypercalcemia, and a variety of medications (eg, lithium,Declomycin).
Clinical Manifestations • Enormous daily output of very dilute, water-like urine. • Intense thirst: The patient drinks 2 to 20 liters of fluid daily. • Fluid intake cannot be limited; otherwise the patient will experience crave for fluid and would develop hypernatremia and severe dehydration.
Assessment and Diagnostic Findings • Fluid deprivation test for 8 to 12 hours. • The patient is weighed frequently during the test. • Perform plasma and urine osmolality studies before and after the test. • Low specific gravity and weight loss, rising serum osmolality, and elevated serum sodium levels. • Terminate the test if tachycardia, excessive weight loss, or hypotension develops. • Plasma levels of ADH (vasopressin) and plasma and urine osmolality.
Medical Management Aims to: • Replace ADH • Ensure adequate fluid replacement • Identify and correct the underlying cause
Pharmacologic Therapy • Desmopressin (DDAVP), a synthetic vasopressin. • Intramuscular administration of ADH. • Clofibrate, a hypolipidemic agent, has an antidiuretic effect. • Chlorpropamide (Diabinese) and thiazide diuretics are used in mild forms of the disease as they potentiate the action of vasopressin. • Thiazide diuretics aand prostaglandin inhibitors (ibuprofen, indomethacin, and aspirin) are used to treat the nephrogenic form of the disease.
Nursing Management of Diabetes Insipidus • Encourage and support the patient while undergoing studies. • Inform the patient and family about follow-up care and emergency measures. • Provide specific verbal and written instructions, and train the patient how to administer the medications. • Advise the patient to wear a medical identification band and to carry medication and information about this disorder at all times. • Vasopressin must be administered with caution if the patient has coronary artery disease because the medication causes vasoconstriction.
Abbreviations • GH: Growth hormone • ACTH: Adrenocorticotropic hormone (Stimulates synthesis and secretion of adrenal cortical hormones) • TSH: Thyroid stimulating hormone (Stimulates synthesis and secretion of thyroid hormone) • FSH: Follicle-stimulating hormone (stimulates growth of ovarian follicle, ovulation; stimulates sperm production) • LH: Luteinizing hormone (production of estrogen and progesterone)