Download
1 / 18
180 likes | 205 Vues
Explore the latest advancements in molecular classification and gene expression profiling of breast cancer, including the benefits of hormonal therapy and gene profiling in treatment decisions. Learn about different signaling pathways in ER+ tumors and the potential of combining anti-estrogen therapy with targeted treatments.

E N D
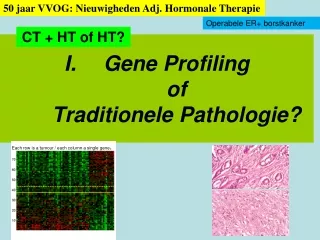
50 jaar VVOG: Nieuwigheden Adj. Hormonale Therapie Operabele ER+ borstkanker CT + HT of HT? Gene Profilingof Traditionele Pathologie? Each row is a tumour / each column a single gene.
Gene Expression Profiling of Breast Cancer (Arrays for mRNA transcripts) • Molecular Classification of Breast Cancer: • Prognostic value and many possible approaches • Top down / Bottom up/ …prognostic signatures • Four main molecular classes of breast cancer have been distinguished! • Luminal A, Luminal B, HER-2, Basal Like
There is a large concordance between all gene-expression based predictors Profiles do quantify mainly tumor proliferation. • intrinsic subtypes (4…) • 70-gene profile, • 76-gene profile, • (wound response) • recurrencescore, • (two-gene ratio) • … 100% agreement Basal like (ER-PR-HER-2-HER-1-CK5,6+ ER-negative, HER-2 positive Veridex 80% concordance between Mammaprint & CellSearch & Oncotype Dx They track different gene sets but the significant agreement in the outcome predictions for individualpatients means they track a common set of biologicphenotypes. All include cell-cycle and proliferation-related genes N Engl J Med. 2009 Feb 19;360(8):790-800. Review.
Mindact-GuidedTherapy In Mindact: 71% in stead of 87% will get chemotherapy! RASTER Lancet Oncol Please look for other markers 30% chemo UZ Leuven: 573 ER+, Grade 2, node negative: 9% had chemotherapy At 5.5 yrs FU 4.3% distant relapse
II. Zijn AIs beter dantamoxifen? 50 jaar VVOG: Nieuwigheden Adj. Hormonale Therapie Operabele borstkanker Postmenopausal Update latest trials BIG 1-98: Letrozole IES: Switch to Exemestane TEAM: Upfront Exem vs Switch
BIG 1-98: Letrozole or Tamoxifen or Switch at Year 2 (NEJM 2009)
2008/9 Highlights in Adjuvant Tamoxifen versus AI ASCO 2009 • Risk-stratification factors are helpful in making treatment decisions • Patients with "higher"-risk tumors -- node-positive breast cancers, tumors that are HER-2 positive and/or lack high levels of ER or PR, or that have high Ki67 scores or bad Mammaprint / Oncotype DX signature may be advised to start with an AI. • For lower-risk, node-negative tumors with other favorable prognostic features, ANY treatment strategy yields a good prognosis. • Patients intolerant to either tamoxifen or an AI can be reassured that the long-term differences between these antiestrogen options remain very small. • If you consider an AI, there might be an additional benefit on DFS when adding a bisphosfonate
QoL: AI versus TAM Against AI • Bone • Joints, CTS • Sexual Health • Cardio-Vascular! Elderly! • Cognitive Function • Gastro-Intestinal Upset • Uterus • DVT • Flashes Against TAM
III. Improving Anti-Estrogen Therapy ER+ Tumors Utilize Different Signaling Pathways Cross Talk between ER and many Growth Pathways Growth Factor Receptors ER-positive The Future GFR Luminal SRC IRS1 PI3Kp85 Frequent PI3K/AKT mutations PI3Kp110 Rictor RAS De Novo Acquired Torc1 PTEN PDK2/mTOR PDK1 RAF AKT Basal ER-negative TSC2 Erk Mek TSC1 More HER-2 signaling if ER+ tumours are PR-negative. HJ Huang et al. BCRT/JCP Stemke-Hale, et al., Can Res 68, 2008
MABs and NIBS: Interfering with Oestrogen Receptor- Mediated Signalling Pathways in Breast Cancer
PFS: Letrozole vs Letrozole + Lapatinib: HER2+ Population 14
Future of Adjuvant anti-E • Who is resistant to tamoxifen? • Gene profiles • Pharmacogenetics • Bisphosfonates if AI for efficacy: Needs Validation? • Extended anti-E beyond 5 years if high risk? • Continuous / Interrupted • AI / Tam / AI versus Tam / AI / Tam • Combining anti-E with targetted therapy in adjuvant? • Tam + Iressa • Anastrozole + Herceptin • Letrozole + Lapatinib • Letrozole + Everolimus* * Neo-adjuvant setting/ 4 months setting
Correspondence between Molecular Class and Clinicopathological Features of Breast Cancer When including Clinico-Pathological Features … N Engl J Med 2009;360:790-800
Prognosis by ER, PR, HER-2All UZ Leuven Consecutive Cases (n=2059) Disease Free Survival (months) 5.4 years after primary operation for breast cancer
IGF-1R, EGFR • Preclinical data show that long term estrogen deprivation (LTED) MCF7 cells exhibit upregulation of ErbB2/MAPK, p-Akt/ p-S6K1/ p-4E-BP1. mTOR pathway plays the primary role in mediating the proliferation of LTED cells. • Combination mTOR inhibition and hormonal therapy↓ cell proliferation and ↑ apoptosis in BC cells to a greater extent than either agent alone4 • mTOR inhibition reverses resistance to hormonal therapy in BC5,6 with synergistic antitumor effects with hormonal therapy7 • Objective responses and stable disease in patients with BC treated with mTOR inhibitors alone1-3 ER RAS PI3K AKT RAF ER TSC1 TSC2 MEK mTOR ERK Cell Growth Metabolism Angiogenesis Cell Proliferation ER 1. Chan et al. J Clin Oncol. 2005;23:5314-5322. 2. Tabernero et al. J Clin Oncol. 2008;26:1603-110.3. Ellard et al. J Clin Oncol. 2007;25(18s):141s. Abstract 3513. 4. Boulay et al. Clin Cancer Res. 2005;11:5319-5328. 5. deGraffenreid et al. Clin Cancer Res. 2004;10:8059-8067. 6. Ghayad et al. Cancer Sci. 2008;99:1992-2003.7. Lisztwan et al. Breast Cancer Res. 2008;10:R56.