
THE PARADOXICAL RBC
E N D
Presentation Transcript
THE PARADOXICAL RBC MEDICINE GRANDROUNDS December 2, 2010 Presented by: Suzanne V. Santos, M.D. Moderator: Jesus A. Relos, M.D., FPCP
Objectives • 1. To discuss the diagnostic approach in a patient presenting with erythrocytosis and thrombocytosis. • 2. To present an unusual case of Beta Thalassemia intermedia with possible concurrent polycythemia vera. • 3. To discuss the pathophysiology, diagnosis and treatment of polycythemia vera and beta thalassemia and their risk for thrombotic events.
General Data • A.B. • 56 year old male • Seaman
Chief Complaint Headache
History of Present Illness 14 years PTC elevated BP 150-160/80 (1995) occasional headache Consultation done: Dx. Hypertension stage II 10 years PTC Dx: Dyslipidemia (2005) Hyperuricemia
History of Present Illness 3 months PTC occipitalheadache, (Oct. 2009) throbbing,grade 5-6/10 consultation: CBC: elevated Hgb (19.3), Hct (60) Blood volume studies Referral to hematologist
No fever • No weight loss • No loss of appetite • No dizziness • No nausea/vomiting • No easy bruisability • No bleeding tendencies • No mouth sores • No skin rashes • No hair loss Review of Systems
Past Medical History • Hypertensive for 14 years Usual BP 120-130/80, Highest BP 160/90 Maintenance: Losartan 100mg/tab, 1 tab OD Amlodipine 10mg/tab, 1 tab OD Imidapril 10mg/tab, 1 tab OD • Chronic Kidney Disease x 1 year, Rx: Sodium Bicarbonate 650mg/tab, 1 tab BID • Dyslipidemia for 10 years Simvastatin 80mg/tab, 1 tab ODHS • Hyperuricemia for 10 yrs, on Allopurinol 300mg/tab 1 tab OD
Personal/Social History • Non-smoker • Occasional Alcoholic Beverage Drinker • No history of Illicit Drug Use
Family History Unremarkable
Physical Examination • BP: 130/90, CR: 74 bpm regular, R: 20 cpm, T: 36.8C • Ht: 167.64 cm, Wt: 68 kg, BMI: 24 kg/m2 • General appearance: conscious, coherent, not in cardiorespiratory distress, ambulatory, oriented to 3 spheres • Skin: flushed, moist skin, no rashes over face or body • HEENT: plethoric, pink palpebral conjunctivae, anicteric sclerae, no nasoaural discharge, no cervical lymphadenopathy, no palpable neck mass, thyroid not enlarged
Physical Examination • CHEST and LUNGS: symmetrical chest expansion, no retractions, clear breath sounds, no crackles or rhonchi, no wheeze • HEART: quiet precordium, apex beat at 5th ICS left mid clavicular line, regular rate and rhythm, no murmurs. No S3, No S4 gallop, S1>S2 apex, S2>S1 base, JVP at 9 cm, distinct heart sounds • ABDOMEN: Flabby abdomen, soft, nontender, normoactive bowel sounds, no hepatosplenomegaly • EXTREMITIES: no cyanosis, no edema, full and equal pulses, no nail changes, no tender or swollen joints • Neurological Examination: essentially normal
Salient Features • 56 year old male • Headache • Elevated blood volume studies • 14 yrs history of elevated BP • 10 yrs history of hyperuricemia • Non smoker • Plethoric • Hgb 19.3, Hct 60
Initial Clinical Impression • Myeloproliferative Disorder probably Polycythemia Vera • Hypertensive Cardiovascular Disease • Dyslipidemia • Hyperuricemia • Chronic Kidney Disease probably secondary to Hypertensive Nephrosclerosis
Definition of Terms • Hemoglobin (Hgb): concentration of the major oxygen-carrying pigment in whole blood; tetramer consisting of a pair of α-like chains andβ-like chains • Hematocrit (HCT): percentage of a sample of whole blood occupied by intact red blood cells. • RBC count: number of red blood cells contained in a specified volume of whole blood. • Erythrocytosis: increased red cell mass • Polycythemia: hemoglobin, red blood cell (RBC) count, and total RBC volume are all above normal.
Definition of Terms • Hemoglobin (Hgb): concentration of the major oxygen-carrying pigment in whole blood; tetramer consisting of a pair of α-like chains andβ-like chains • Hematocrit (HCT): percent of a sample of whole blood occupied by intact red blood cells. • RBC count: number of red blood cells contained in a specified volume of whole blood. • Erythrocytosis: increased red cell mass • Polycythemia: any increase in red cells Men: Hgb > 17 g/dL; Hct > 50% Women: Hgb > 15 g/dL; Hct > 45%
Definition of Terms MCV: volume of the average circulating RBC MCH: hemoglobin content of the average circulating RBC MCHC: hemoglobin concentration within circulating RBC Microcytosis: MCV < 80 Macrocytosis MCV >100 Hypochromia: low values of MCH and MCHC
Problem: Erythrocytosis & Thrombocytosis • Phlebotomy: 1st consult (2/3/09) 3rd consult (2/5/09) 10th consult (2/12/09)
Complete Blood Count 2/11/10
Problem: Erythrocytosis & Thrombocytosis Cranial CT scan without contrast: (Feb. 16, 2010) Suspicious small infarct, anterior limb of the right internal capsule. Microvascular disease. Atherosclerotic disease of the vertebro-basilar and internal carotid arteries.
Problem: Erythrocytosis & Thrombocytosis WHO Classification of Chronic Myeloproliferative Disorders (Neoplasm) • Chronic Myelogenous Leukemia • Chronic Idiopathic Myelofibrosis • Essential Thrombocytosis • Polycythemia Vera
Problem: Erythrocytosis & Thrombocytosis WHO Classification of Chronic Myeloproliferative Disorders • Chronic Myelogenous Leukemia • Chronic Idiopathic Myelofibrosis • Polycythemia Vera • Chronic Myelogenous Leukemia • translocation between chromosome 9 and 22 resulting in fusion of the BCR gene on chromosome 22q11 with the ABL gene on chromosome 9q34 • elevated WBC, plt count • low LAP score • Patient • Detection of BCR-ABL Gene Fusion by FISH (4/12/10): 1% found positive • normal WBC • high LAP score at 189
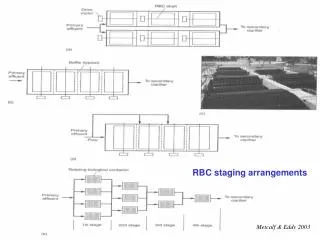
Problem: Erythrocytosis & Thrombocytosis WHO Classification of Chronic Myeloproliferative Disorders • Chronic Myelogenous Leukemia • Chronic Idiopathic Myelofibrosis • Polycythemia Vera • Chronic Idiopathic Myelofibrosis • marrow fibrosis, extramedullary hematopoiesis, splenomegaly • Blood smear: teardrop-shaped red cells, nucleated red cells, myelocytes, promyelocytes • Patient • Bone Marrow Biopsy done 3/31/10
A.B. 56/Male 10-2949 BM
Problem: Erythrocytosis & Thrombocytosis Bone Marrow, Core Biopsy and Aspirate Smears (3/31/2010) Normocellular bone marrow (40-50%) with orderly trilineage hematopoiesis.
Problem: Erythrocytosis & Thrombocytosis WHO Classification of Chronic Myeloproliferative Disorders (Neoplasm) • Chronic Myelogenous Leukemia • Chronic Idiopathic Myelofibrosis • Essential Thrombocytosis • Polycythemia Vera • Essential Thrombocytosis • Elevated platelet count • hemorrhagic and thrombotic tendencies • mild neutrophilic leukocytosis • normal or elevated LAP score • Bone marrow biopsy reveals megakaryocyte hyperplasia and hypertrophy with increase in marrow cellularity • Patient • Platelet count not consistently elevated • elevated LAP score • Normal bone marrow biopsy
Problem: Erythrocytosis & Thrombocytosis Polycythemia Vera Study Group (PVSG) • increased red blood cell mass (red cell volume > 36ml/kg) or increased hgb or hct • Disorders causing secondary erythrocytosis are absent. PVSG criteria: two basic criteria plus 2 of the ff.: • Platelet count >400,000/microL • White blood cell count >12,000/microL • LAP score greater than 100 • Presence of a JAK2 gene mutation • Bone marrow biopsy showing hypercellularity with prominent erythroid, granulocytic, and megakaryocytic proliferation
Problem: Erythrocytosis & Thrombocytosis Polycythemia Vera Study Group (PVSG) • increased red blood cell mass (red cell volume > 36ml/kg) or increased hgb or hct • Disorders causing secondary erythrocytosis are absent. PVSG criteria: two basic criteria plus 2 of the ff.: • Platelet count >400,000/microL • White blood cell count >12,000/microL • LAP score greater than 100 • Presence of a JAK2 gene mutation • Bone marrow biopsy showing hypercellularity with prominent erythroid, granulocytic, and megakaryocytic proliferation
Problem: Microcytic and Hypochromic RBC • Genetic Studies (May 6, 2010): No apparent chromosomal abnormality • Thalassemia Screening in the Philippines using High Performance Liquid Chromatography (HPLC) (July 9, 2010): HPLC tracing is indicative of beta-thalassemia, intermedia
Polycythemia Vera • Most common of the myeloproliferative disorders • Incidence: 2 per 100,000 persons Etiology: Unknown • nonrandom chromosome abnormalities such as 20q, trisomy 8, and 9p • JAK2 V617F mutation causing constitutive activation of the kinase
Janus Kinase2-gene (JAK2) • Janus Kinase 2 (JAK2) has tyrosine kinase activity and is involved in signal transduction from EPOR (erythropoietin receptor) to nucleus for gene expression
Polycythemia Vera: Clinical Features • Splenomegaly • Elevated Hgb and Hct • Neurologic symptoms: vertigo, tinnitus, headache, visual disturbances, TIAs • Systolic hypertension • Venous or arterial thrombosis • Intraabdominal venous thrombosis • Digital ischemia, easy bruising, epistaxis, acid peptic disease or GI hemorrhage
Polycythemia Vera: Diagnosis • Erythrocytosis, leukocytosis, thrombocytosis • Increased leukocyte alkaline phosphatase (LAP) score • Hyperuricemia • Elevated Vit B12 or B12 binding capacity • BMA: no specific diagnostic information • No specific cytogenetic abnormality
Polycythemia Vera: Complications • Increase in blood viscosity • Increased turnover of red cells, leukocytes and platelets with the attendant increases in uric acid and cytokine production • Spleenic infarction • Increased incidence of acute nonlymphocytic leukemia • erythromelalgia
Polycythemia Vera: Treatment • Phlebotomy or bloodletting has been the mainstay of therapy. • Elevated platelet counts may be exacerbated by phlebotomy, thus is an indication to use myelosuppressive agents to avoid thrombotic or hemorrhagic complications.
Polycythemia Vera: Treatment Hydroxyurea has been the mainstay therapy after the PVSG results indicated it as an effective agent for myelosuppression. The role of HU in leukemic transformation is not clear, but several nonrandomized studies have supported or refuted a significant rise in leukemic conversion with long term use of HU in persons with polycythemia vera (from 2.1% to 10%). Besa, Emmanuel, M.D., and Woermann, Ulrich, M.D. Polycythemia Vera: Treatment and Medication. January 23, 2009.
Thalassemia Syndromes • Inherited disorders of α or β globin biosynthesis, diminished production of Hgb tetramers • Unbalanced chain accumulation • Massive bone marrow expansion deranges growth and development (“chipmunk” facies) • Chronic transfusion leads to iron overload
Thalassemia Syndromes • α Thalassemia • β Thalassemia
β Thalassemia • β Thalassemia Major: either no effective production or severely limited production of beta globin. • β Thalassemia Minor: heterozygotes who have inherited a single gene leading to reduced beta globin production. • β Thalassemia Intermedia: disease of intermediate severity, such as those who are compound heterozygotes of two thalassemic variants.
β Thalassemia Intermedia • Malaise, pallor, easy fatigability, splenomegaly • CBC reveal anemia with marked hypochromasia and microcytosis • Accepted Hgb: 6-7 g/dL without blood transfusions. • Treatment: close monitoring and observation. • Indications for blood transfusions: intercurrent infections, hypersplenism, or other illnesses.
β Thalassemia Minor and Newly Diagnosed Polycythemia Rubra Vera in a 71- year old WomanJason Preston Thomas, M.D.Hospital Physician April 2001 • β Thalassemia Minor and polycythemia rubra vera (PRV) are hematologic disorders that give opposite results and the 2 disease entities occurring simultaneously has only been reported ONCE. • Due to the low-grade hemolysis resulting from precipitation of impaired alpha globin chains in association with β Thalassemia Minor, the often substantial elevations in Hgb and Hct seen in PRV were probably blunted. • The low grade anemia of β Thalassemia Minor is not evident because of the overproduction of erythrocytes.
Final Diagnosis • Myeloproliferative Disease probably Polycythemia Vera • Beta Thalassemia Intermedia • Hypertensive Cardiovascular Disease • Dyslipidemia • Hyperuricemia • Chronic Kidney Disease probably secondary to Hypertensive Nephrosclerosis
Complete Blood Count 10/2/10