
Case of The Week
E N D
Presentation Transcript
History • 52 years old women presented with 3 weeks history of progressive abdominal pain, diarrhea, weakness, fatigue and weight loss of few kilograms. 18 days earlier she undergone left total knee replacement that was complicated by left DVT. 4 days after heparin therapy she developed abdominal pain, tachycardia and transient hypotension. There was a fall hematocrit and platelets with no apparent source of bleeding. IVC filter was inserted and she was discharged home on analgesics in stable state
On Examination: • Pulse 90 bpm, BP 98/48 lying, 86/54 standing, RR 20 bpm, T 36.3 °C • The patient looked ill; well-healed darkly-pigmented right knee scar was noted. Rest of physical exam was unremarkable. Laboratory findings: • Hemoglobin 12 g/l, Na+ 134 mmol/l, K+ 5.6 mmol/l, creatinine 65 umol/l
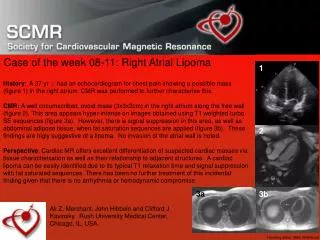
Enlarged adrenal gland with clear high signal intensity of the right adrenal gland in (image 1) and mixed signal intensity of the left adrenal gland, indicative of recent bilateral adrenal hemorrhage.
Mention some other causes that may cause this particular condition.
Systemic sepsis _ Waterhouse –Friderichsen syndrome • Primary anti-phospholipids antibody syndrome • Disseminated intravascular coagulation (DIC) • Congestive heart failure
What is the final diagnosis? Elaborate on the clinical scenario that led to this condition.
Heparin induced coagulation defect complicated by bilateral adrenal hemorrhage • Subsequent acute adrenal insufficiency was overlooked initially due the non- specific nature of symptoms: abdominal pain, tachycardia and hypotension
Elaborate on the management of this condition , including information supplied to the patient regarding therapy.
Blood sample for cortisol, ACTH, aldosterone, and plasma renin activity(PRA) should be obtained. • Replacement therapy with steroid and supportive therapy to correct water and electrolytes deficits. • Correction of underlying condition. • Patient should be informed to double or triple dose of oral corticosteroids therapy with any minor illness. Major illness demands patient to self-inject hydrocortisone (100 mg) and promptly seek medical advice.
Adrenal Hemorrhage • Introduction • Adrenal hemorrhage is a relatively uncommon condition with a variable and non-specific presentation that may lead to acute adrenal crisis, shock, and death unless it is recognized and treated appropriately.
Incidence • Adrenal hemorrhage has been reported in 0.3-1.8% of unselected cases in autopsy studies, although extensive bilateral adrenal hemorrhage may be present in 15% of individuals who die of shock. • It’s more common in males (male-to-female ratio of 2:1), probably reflecting a male predilection for several of the underlying conditions associated with adrenal hemorrhage.
Etiology 1) Infection : sepsis ,wound infection Waterhouse-Friderichsensyndrome (purpurafulminans) : represents hemorrhagic necrosis of several organs associated with meningococcal disease,streptococcus pneumoniae and other organism 2) Cardiac : Myocardial infarction , congestive heart failure 3) Blunt trauma
Etiology cont. 4) Hemorrhagic disease With anticoagulant use, thrombocytopenia, and vitamin K deficiency 5) Vascular : Arterial: CVA, peripheral arterial embolization Venous: DVT, superficial thrombophlebitis Primary anti-phospholipids antibody syndrome 6) Adrenal : Amylodosis, metastatic cancer
Adrenal Hemorrhage • Pathogenesis • Its pathologic characteristics typically include bilateral gland involvement with extensive necrosis of all 3 cortical layers and of medullary adrenal cells. • adrenal vein spasm induced by high catecholamine levels secreted in stressful situations and by adrenal vein thrombosis induced by coagulopathies may lead to venous stasis and hemorrhage. • Furthermore, in stressful situations, ACTH secretion increases, which stimulates adrenal arterial blood flow that may exceed the limited venous drainage capacity of the organ and lead to hemorrhage
Symptoms • Symptoms of adrenal hemorrhage are non-specific • abdominal, lumbar, pelvic, or thoracic pain which is the most consistent feature. • symptoms of acute adrenal insufficiency, such as fatigue, anorexia, nausea, and vomiting.
Symptomscont. • Symptoms of the underlying condition(s) predisposing to adrenal hemorrhage may be present. For example, patients with Waterhouse-Friderichsen syndrome often experience prodromic, non-specific symptoms, including malaise, headache, dizziness, cough, arthralgias, and myalgias.
Clinical manifestation Depend on the on the extent of adrenal hemorrhage, the bleeding rate, and the underlying cause, as well as according to whether the adrenal hemorrhage is bilateral or unilateral. 1) Fever (>38 °C) (50-70%) vary from low grade fever to high fever with chills 2) Tachycardia 3) Orthostatic hypotension 4) Shock Sepsis, Waterhouse-Friderichsen syndrome, Hypovolemia
Clinical manifestation 5) Hypertension In the presence of unilateral adrenal hemorrhage 6) Petechial lesions In the case of Waterhouse-Friderichsen syndrome 7) Confusion and disorientation 8) Acute abdomen 9) Skin hyper-pigmentation Which occur with Chronic adrenal insufficiency
Investigations *Laboratory studies: 1) Complete Blood Count : • Decrease in Hb and Hct • Leucocytosis 2) Serum Electrolyte : - Hyponatermia and Hyperkalemia • Hypoglycemia 3) Serum cortisol, plasma ACTH, serum aldosterone, and plasma renin activity (PRA) 4) The short Cortrosyn stimulation test
Investigation *Imaging studies: 1) CT Scan: -useful in hemodynamicallysatble patient -Initially the gland has rounded or oval shaped and may be asymmetric. -Later on it has a cystic appearance . -After several weeks the gland shows a gradual decrease in adrenal size . -After several months the adrenals shows progressive atrophy, with the variable appearance of calcifications
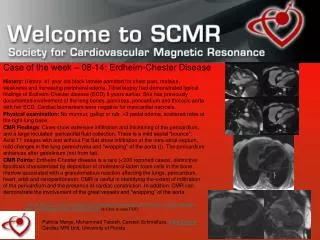
Computed tomographic (CT) scans of the abdomen show normal adrenal glands several months before the onset of hemorrhage (upper panel) and enlarged adrenals 2 weeks after an acute episode of bilateral adrenal hemorrhage (lower panel). The attenuation of the adrenal glands, indicated by arrows, is increased after the acute event.
Investigation 2) MRI: -It’s used to exclude the presence of malignant tumors or pheochromocytomas . -It may provide an estimate of the age of the hematoma 3) Ultrasound: - It may reveal a hyperechoic masses that contain central echogenic area in the adrenal gland .
Management 1) Treat the cause 2) Replace adrenal function 3) Provide vital support 4) Correct electrolyte disturbances 5) Surgical intervention
Prognosis • The acute case fatality rate associated with extensive, bilateral adrenal hemorrhage is approximately 15% and varies according to the severity of underlying illness. • Waterhouse-Friderichsen syndrome, the case fatality rate is 55-60%, particularly when the diagnosis is delayed. Death occurs from sepsis, despite appropriate antibiotic, glucocorticoid, and supportive treatment. • Recovery of adrenal function in patients with chronic adrenal insufficiency associated with adrenal hemorrhage is possible, although it appears to occur infrequently
References 1)Adrenal Hemorrhage :Nicholas A Tritos, MD, DSc, MMSc, FACE, FACP, Assistant Professor of Medicine, Tufts University School of Medicine; Senior Staff Physician, Department of Endocrinology, Lahey Clinic Medical Center