Download
1 / 22
220 likes | 393 Vues
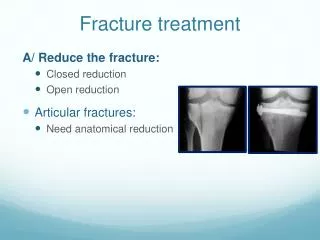
Fracture treatment. A/ Reduce the fracture: Closed reduction Open reduction Articular fractures: Need anatomical reduction. Fracture treatment. A/ Reduce the fracture: Closed reduction Open reduction Articular fractures: Need anatomical reduction Diaphyseal fractures

E N D
Fracture treatment A/ Reduce the fracture: • Closed reduction • Open reduction • Articular fractures: • Need anatomical reduction
Fracture treatment A/ Reduce the fracture: • Closed reduction • Open reduction • Articular fractures: • Need anatomical reduction • Diaphyseal fractures • Need functional reduction • Restore length, axis, and rotation
Fracture treatment B/ Hold reduction until healing: • Methods of holding reduction • Sustained traction • Cast splint • Functional bracing • Internal fixation • External fixation
Fracture Management • Treatment of closed fractures • Treatment of open fractures Different
Treatment of closed fractures • Emergency care (splinting) • Definitive fracture treatment • Rehabilitation • muscle activity and early weightbearing are encouraged
Emergency care (splinting) • Splint them where they lie • Adequate splinting is desirable • Type of splints: • Improvised • conventional
Conservative • Reduction: (if displaced) • under general anasthesia, the sooner the better • Steps of Reduction: • Traction • Align (which fragment) • Reverse mechanism of injury • Immobilization: • POP (Plaster of Paris) cast, slab, traction • Rehabilitation
Closed reduction • Traction in the line of the bone • Pressing fragment into reduced position • Disimpaction
Indications of Open reduction • Absolute: • when closed reduction fails • when there is an articular fragment that needs accurate positioning • for traction (avulsion) fractures in which the fragments are held apart • Relative: • Multiple fractures • Pathological fractures • To encourage early mobilization and avoid joint stiffness. e.g. Diaphyseal fractures
Type of internal fixation • Screws • Wires • Plates and screws • Intramedullary nails
External fixation • Indications in acute trauma: • Fractures associated with severe soft-tissue damage(including open fractures) or those that are contaminated • Fractures around joints that are potentially suitablefor internal fixation but the soft tissues are tooswollen to allow safe surgery • Patients with severe multiple injuries
Rehabilitation • Restore function of the • injured parts and, • patient as a whole • The objectives are: • to reduce edema • preserve joint movement • restore muscle power • guide the patient back to normal activity
Treatment of open fractures • The four essentials are: • Antibiotic prophylaxis • Urgent wound and fracture debridement • Stabilization of the fracture • ? External Fixation • Early definitive wound cover To be discussed separately
Complications of Fractures • Nonunion (failure to heal) • 3% overall • 50% of some particular fractures • Related to treatment, local problems, systemic problems (e.g. Smoking)
Complications of Fractures • Malunion: (Healing in poor position) • Deformity • Risk of arthritis
Complications of Fractures • Fat embolism syndrome • Marrow elements (fat) released into the vascular system and travel to the lungs • Triglycerides (fat) metabolized to FFA by pneumatocytes and these FFS are toxic to tissue • Especially brain, blood vessels, kidneys • ARDS • Risk of death
Fat Embolism • Diagnosis • ARDS • Mental status changes • Petechial hemorrhage • Other • Treatment • Respiratory Support • Early recognition
Complications of Fractures • DVT/Pulmonary embolism • Fracture leads to immobilization • Stasis, hypercoagulability, intimal injury • Thrombosis of LE veins • Embolism to heart and then lungs • Mechanical blockage • Ventilation/perfusion mismatch
DVT Prevention • Mobilization • Patient • Limb • Mechanical • Skeletal stabilization • SCD, foot pumps • Compression • Chemical anticoagulation
Pitfalls in Fracture Management • History of mechanism of injury not obtained • Combination injury missed • Soft tissue not considered • Failure to consider occult fractures • X-rays not proper; exposure, views.. • Inadequate film accepted
Summary • What is a Fracture – the soft tissue part • Fracture types • Relation between fracture and force • How fractures heal • Principles of imaging • Principles of treatment • Complications of fractures