Download
1 / 53
530 likes | 791 Vues
Women and Heart Disease. Cathryn Harbor Lexington VA May19,2004 Sponsored by National Organization for Women. Coronary Artery Disease. Definitions. Heart Attack: Heart Muscle is damaged because it cant get blood and oxygen.

E N D
Women and Heart Disease • Cathryn Harbor • Lexington VA • May19,2004 • Sponsored by National Organization for Women
Definitions • Heart Attack: Heart Muscle is damaged because it cant get blood and oxygen. • Angina: Heart Muscle is deprived of blood flow and oxygen. A charlie horse.
Statistics • Disease of Arteries is the leading cause of death. • After menopause women develop heart disease at the same rate as men. • After menopause, women are 10 times more likely to develop heart disease than to develop breast cancer. • 40% of people who have a heart attack die of it.
Life Cycle Differences • Young women develop less disease in the heart arteries than young men. • After menopause, a woman’s arteries develop disease at a similar rate to men’s.
Heart Disease in Women vs Men • After menopause women are equally susceptible • Men have more chest pain. Women more often have “silent” heart attacks • Once diagnosed women do worse
Red Flag Symptoms • Chest Pain or Pressure • Dizziness • Shortness of Breath • Neck Pain unassociated with neck movement • Any Unusual Symptom that occurs with exertion and resolves with rest • Unexplained Sweats • Nausea
What to do if you have symptoms • Take an asprin • Stop any exertion • Go to the ER if the symptom persists. If it resolves, contact your health care provider.
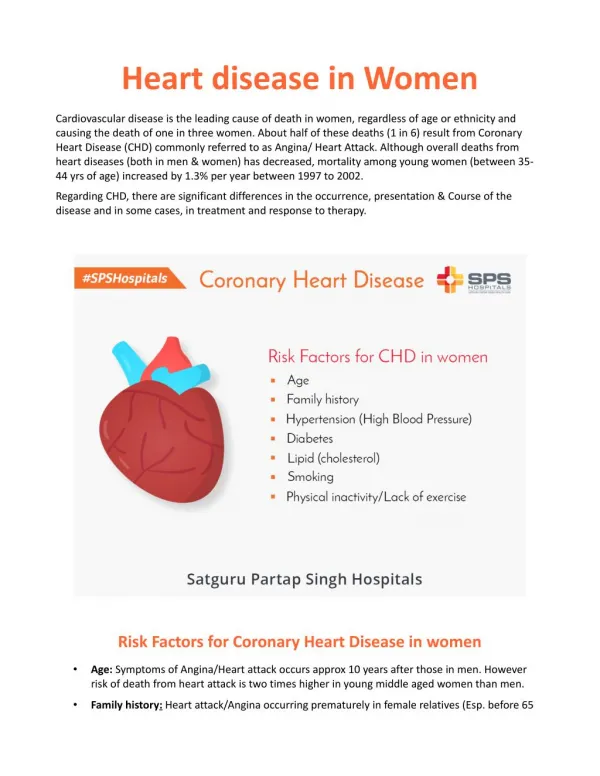
Known risk factors • There are more than 80 known risk factors for heart disease • This means that there is no one cause and no one treatment.
Smoking Being overweight Age Hypertension Diabetes Physical Inactivity Elevated cholesterols Elevated C Reactive Protein Elevated Fasting Blood Sugar (90) Stress, anxiety, depression Elevated homocysteine Important Risk Factors
Genetic Contribution • We know that genetics plays a big role • .Genes tell your body how to make proteins, that is all. To have a genetic problem simply means that you inherit the blueprint for less effective proteins. It does not mean that you inherit heart disease. • No genetic factors I have found that are not modifiable by environment
The Problem of Choice • Hard to know what to do. • Science does not provide clear answers • Science does not progress rapidly • What is driving the science?
Women and Heart Health: Choices • Should I use hormone replacement? • Should I use medicines to lower my cholesterol? • Should I change my lifestyle?
Women and Hormones:What We Do Know • Before menopause women’s risk of heart disease is much lower than men’s. • After menopause, women’s risk quickly approaches men’s. • In large surveys women who take estrogen after menopause have less heart disease (nurse’s study).
Evolution of HRT • Drug companies started producing estrogen from pregnant mare’s urine (Premarin). • Studies showed that estrogen without progesterone causes uterine cancer. • Drug companies started making combination packages of estrogen and progestins. • Because of Patent issues, the progestins the drug companies used were not natural to the body, but synthetic.
Evolution of HRT continued • Because of the belief, based on good studies, that HRT protects against heart disease, women were told at menopause that they should start premarin to protect their hearts. • Premarin became the most widely prescribed drug in the country
HERS trial • 2763 postmenopausal women • Pre-existing heart disease • Randomized to placebo or prempro • 4.1 year study
HERS Trial Results • In the first year more women on prempro group had more heart attacks than women in the control group • For the 2nd and 3rd years the groups very similar • By the 4th year more women in the control group had heart attacks
Impression after HERS Trial • Starting on HRT after heart disease is established is dangerous at first • After a few years on HRT estrogen use seems to create no additional risk and possibly to protect women
What Would Explain the Results of HERS? • We know that estrogen increases women’s chance of forming clots in our blood vessels • Women in the trial were known to already have diseased arteries. • Possibly starting a woman on HRT after she has developed heart disease was the problem, since a clot is a bigger problem in a sickened and narrowed artery.
THE WOMEN’S HEALTH INITIATIVE (WHI) • 16,608 post menopausal women without hysterectomy not currently on HRT • Randomized to placebo or prempro • Planned duration 8 years • Stopped by safety advisory board after 5.3 years: “increased risk of breast cancer without evidence of overall benefit”.
FINDINGS OF WHI • Breast cancer, heart disease, stroke, lung clots and leg clots are all increased by prempro (in this population). Prempro may have more negative effects than estrogen alone • Hip fractures and colorectal cancer are reduced by prempro (in this population) • Prempro increased the risk of hysterectomy
Problems with WHI • WHI intentionally excluded women with severe menopausal symptoms, though these women are most likely to use HRT. • Older women not on HRT were studied. Many of them can be presumed to already have heart disease. • The study was too short to show benefits, if any, of HRT.
What we STILL Don’t Know • Is there a heart benefit to giving HRT starting right at menopause, before heart disease starts to develop? • Do other types of estrogen and progesterone have same risks? • What if lower doses had been used? • Do older women on hormones need to come off of them?
Take away • We still do not have enough information to make perfect decisions about putting women on or taking them off estrogen • Right now the pendulum has swung very far to the no HRT side.
Cholesterol • People who die of heart attacks have changes in their heart arteries that are made, in part, of cholesterol.
Where Does Cholesterol Come From? • We thought cholesterol in diet made cholesterol in the body. • In fact cholesterol is so important that the body makes its own. • Cholesterol is the result of interactions between carbohydrates, fats and protein in a diet, level of exercise, heredity and hormones.
Cholesterol’s Function • Important in producing hormones • Forms insulation around nerves to keep signals moving • Needed to maintain cell membrane fluidity • Has important immune functions (fighting illness) • Necessary for brain function (thinking) • Important in neurotransmitter production (mood)
About Cholesterol • We usually measure three types of cholesterol: • LDL (bad cholesterol) • HDL (good cholesterol) • Triglycerides
Traditional Approach • Focused on evidence-based medicine • Five major studies showed impressive risk reduction from using statins (24-39% reduction). • Drug trials using statins (Lipitor, Pravacol, Baycol, and Zocor, etc demonstrated both a lowering in LDL cholesterol and a lowering of heart attacks.
Statins some more of the issue • 61-76% of patients treated with statins STILL experience heart attacks.
Lipids and Women • LDL (Bad Cholesterol) is a good predictor of heart disease in men. • Simple LDL measurements predict little in women. • Despite awareness of other modifiable risk factors, we tend to focus on one risk factor (LDL cholesterol) and one therapy (statin drugs)
Tangent about problems with LDL • LDL is clearly bad, at least for men but there are differences among the types of LDL • My LDL is 180 yours is 120. Who has the worst problem? We don’t know because • Answer: It depends on number of cholesterol particles and therefore on the size of the LDL particle.
This Just In • “Women without coronary artery disease do not benefit from Statin use”. • For women with known cardiovascular disease, treating hyperlipidemia is effective in reducing fatal and non fatal heart attacks…but “does not affect total mortality”.
Another Big Problem • Coenzyme Q-10 is a very important anti-oxidant. • Coenzyme Q-10 is produced in the body, in the same chemical pathway as cholesterol. • The enzyme, HMG CoA reductase is essential for producing CoQ-10. • Statin drugs work by disabling this enzyme.
CoQ-10 • Many of unpleasant effects of statin drugs (muscle aches, fatigue) can be reversed by using CoQ-10. • CoQ-10 has now been demonstrated to be important in treating Parkinson’s disease. • I believe that everyone on statin drugs should take CoQ-10.
HDL Cholesterol • HDL (good cholesterol) is very important in women: • HDL below 50 makes women 2.7 times more likely to die of a heart attack.
Triglycerides • Triglycerides between 200 and 400 increase risk of heart attack death by 2.4 • Triglycerides above 400 make women 6.9 times more likely to die of heart attacks.
The Metabolic Syndromealso called INSULIN RESISTANCE • Abnormal cholesterol profiles High TG, low HDL high LDL • Hypertension • Type 2 Diabetes • Coronary artery disease • Breast, prostate and colon cancer • Polycystic ovarian disease
Insulin’s Role • High blood sugar is highly toxic to brain tissue. • When you eat carbohydrates your body turns them into sugar, glucose. • Insulin rises after you eat carbohydrates to protect your tissues from excess energy. • Insulin lets excess energy be quickly cleared from the bloodstream to be stored as triglycerides and cholesterol. • In the short term, high insulin levels protect your tissues • In the long run, high insulin levels are associated with many health problems, called the metabolic syndrome.
Triglycerides, Insulin and Diabetes • Learn and control your triglyceride number • Of all lipid markers, this one is associated with the effectiveness of your diet and exercise program. • Triglycerides are where your body stores excess carbohydrate calories • We have long known that Triglycerides are an important marker for CAD risk in women.
A complex problem without an easy solution • What’s a girl to do?
How do you protect yourself? • Lower your risk for heart disease by 70%!
The Lyons Study • 605 French men and women who had survived heart attacks • Divided into two groups: • American heart Association Diet (low fat) • Mediterrainian diet: • Olive oil • Whole grains • More root and green vegetables • More fish and poultry, less red meat
Lyon s Study Results • Study was stopped after only 30 months: • A 70% reduction in deaths from all causes in the group with the Mediterainian diet. • This was in people who had already had heart attacks!
Changes you can make for risk reduction • Stop or avoid smoking • Improve your diet (the LYONS Study) • Maintain a normal weight • Exercise • Consider hormone replacement • Maintain normal blood pressure • Reduce stress in your life
ONE SIZE FITS ALL MEDICINE IS THE BEST FOR THE DRUG COMPANIES. • It is not necessarily the best for your body