SPINAL CORD INJURIES
SPINAL CORD INJURIES. Dr Anba Soopramanien Consultant in Spinal Injuries and Rehabilitation Medicine Glenside Hospital for Neuro -Rehabilitation Visiting Fellow, Bournemouth University. TAKE HOME MESSAGES. Epidemiology: poor statistics

SPINAL CORD INJURIES
E N D
Presentation Transcript
SPINAL CORD INJURIES Dr Anba Soopramanien Consultant in Spinal Injuries and Rehabilitation Medicine Glenside Hospital for Neuro-Rehabilitation Visiting Fellow, Bournemouth University.
TAKE HOME MESSAGES • Epidemiology: poor statistics • Importance of thorough clinical examination • Causes: changing picture • Pathology: many systems are affected. • Prognosis: depends on severity of injuries, associated injuries, quality of rehabilitation. • Support to patients, families and friends crucial.
EPIDEMIOLOGY • Incidence 20 per million in UK for trauma- estimate only In addition: inflammatory, neoplasic vascular Origin- incidence is unknown. • Prevalence About 40,000 people live with SCI in UK • Age Most injuries affect young males, but age increasing. Majority now: tetraplegia and incomplete.
PATHOLOGY Spinal Shock Respiratory system • chest complications • paralysis of ventilatory muscles affecting breathing and coughing capability • relative bronchoconstriction • excess secretions due to relative • parasympathetic system dominance (from reduced sympathetic function in tetraplegics) • ventilation/perfusion mismatch from reduced mobility that may exacerbate hypoxia during • intercurrent illness. Cardiovascular system • symptomatic bradycardiaand, asystolic cardiac arrest, during the acute phase. • loss of sympathetic activity with preservation of parasympathetic (vagal) activity. • Bradycardiausually resolves several weeks after injury during suctioning. • Hypotension (eg 80/50) and • Low pulse rate (eg 40–50 bpm) can be physiologically 'normal' for that level of spinal cord lesion • Overzealous fluid resuscitation…pulmonary oedema ' normal resting vital signs before • Autonomic dysreflexia (AD) – an excessive autonomic response to stimuli. iThisis an acute and life-threatening condition
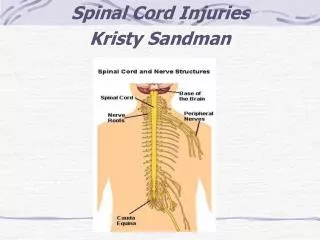
PATHOPHYSIOLOGY • Neurological system • Sensation • Sensory loss will complicate the presentation of acute illness in individuals with SCI as the history will not necessarily include localising symptoms or pain, and • localising signs may not be present.
PATHOPHYSIOLOGYBLADDER • Bladder • Depend on the grade and level of injury. • Urinary tract infections are one of the most common complications The goals of bladder management are to preserve the upper tracts, minimise lower tract complications and compatible with the individual's lifestyle. • ACUTE: Indwelling catheter or SICs • LONG TERM: intermittent self-catheterisation (ISC) regimens, Long-term indwelling urethral catheters …complications: infection or urethral Stricture. • Condom • IncompleteSCI who has some spontaneous voiding but retains a residual volume which gradually increases: this can eventually lead to complications if not appropriately • managed
PATHOPHYSIOLOGY:BOWELS • Bowel • Profound impact on the function of the large bowel and on faecal continence. Stool transit through the bowel is slowed, placing individuals at high risk of • constipation, especially where morphine or codeine related drugs or anticholinergics are used to control • Sensory and motor control of the anorectum is • impaired and therefore individuals will be unable to • feel the need to evacuate the bowel, or control the • process of defaecation. Without intervention, • …. Potential is risk of autonomic dysreflexia, in patients with lesions • above the level of T5–6.
OTHER ISSUES • PAIN: MS pain and neuropathic pain… • GD ULCERS: Now reduced with use of PPIs • DVT & PE: Prophylactic anticoagulation • SKIN: Skin care: Incidence in acute hospitals. • JOINTS & LIMBS: Avoid contractures. • BIOCHEMICAL: Hyponatraemia, Hypercalcaemia, HO, Spasticity. • ASSOCIATED INJURIES: Head (12%), Limb, Chest (19%), Abdominal. • PSYCHOLOGICAL ADJUSTMENTS
PROGNOSIS Depends on severity of injury management in acute stage Do no harm Skin Bladder Bowels SF & FERTILITY