Download
1 / 11
110 likes | 449 Vues
DECREASED URINE OUTPUT (Oliguria). Artak Labadzhyan Mini-Lecture Powerpoints 1/30/12. OBJECTIVES. Definition of decreased urine output (oliguria) Questions to consider when first presented with oliguria Recognizing causes of oliguria Focused review of history and physical

E N D
DECREASED URINE OUTPUT (Oliguria) Artak Labadzhyan Mini-Lecture Powerpoints 1/30/12
OBJECTIVES • Definition of decreased urine output (oliguria) • Questions to consider when first presented with oliguria • Recognizing causes of oliguria • Focused review of history and physical • Management of oliguria • Recognizing life threatening complications
DEFENITION • Oliguria = Urine output <400cc/day (<20cc/hr) • Another def: urine output <0.5ml/kg/hr • Anuria = no urine output • Can signify complete mechanical obstruction of bladder outlet or a blocked Foley
QUICK CONSIDERATIONS • Does the pt have a foley catheter? NO YES FLUSH FOLEY CATHETER WITH 30-50CC NS OBTAIN PVR (w/ US or cath [will provide urine sample]) URINE OUTPUT IMPROVED? PVR ≥ 100? (≥ 50 in younger pts) YES NO YES NO FOLEY LIKELY CLOGGED WITH SEDIMENT PROCEDE WITH FURTHER MANAGEMENT START FOLEY & PROCEDE W/ FURTHER MANAGEMENT PROCEED WITH FURTHER MANAGEMENT
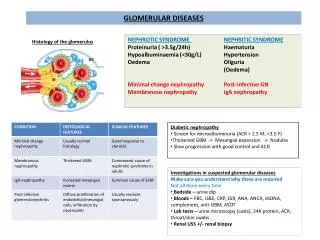
PATHOPHYS • Consider the pathophysiology/causes of decreased urine output. Three categories of causes: • Prerenal: • Volume depletion/dehydration/inadequate fluid maintenance/Infection/sepsis • Reduced cardiac output • ICU setting: mechanical ventilation can also lead to low cardiac output • Drugs • Does the pt have liver cirrhosis • Intrarenal: • ATN • ICU settings: Circulator shock, severe sepsis, multiorgan failure • AIN • Renal artery thrombosis/Emboli (septic [endocarditis] • Postrenal: • B/l ureteric obstruction (stones, clots, tumors, fibrosis) • Bladder outlet obstruction (BPH, tumors/retroperitoneal mass, clots) • Foley catheter obstruction
CHART REVIEW • Review chart to look for clues that may elicit etiology (see previous slide) • History (sepsis, CHF, tumors, renal failure…etc) • Meds: diuretics, ace, aminoglycosides/vancomycin, iv contrast, NSAIDs • Old Labs: BUN/Cr (ratio); urine lytes; blood cultures; vanco trough levels
EXAMINE THE PATIENT • Obtain new vitals, including orthostatics • Look for: • Jaundice • Crackles, pleural effusion • JVP, CVP if pt has central line • Especially useful in ICU for pt with central line: for example a CVP of 2 can be good evidence for hypovolemia • Palpate Kidneys and Bladder • Prostate/Cervical Exam • Rash
MANAGEMENT (Early) • If not already done, order basic electrolytes, CMP (monitor changes in Cr/GFR), and urine studies (U/A, Na, BUN, Cr), to further help classify etiology • Adjust/replace/discontinue and nephrotoxic agents. Also, renally dose the non-toxic meds
MANAGEMENT (Life threatening complications) • Early recognition and intervention of potential life threatening complications (direct or indirect causes – e.g. renal failure) is essential • Hyperkalemia: obtain EKG if elevated • CHF/Pulmonary Edema • Metabolic acidosis; Uremia (encephalopathy, pericarditis) • Advanced complications of above may require dialysis
MANAGEMENT cont… • Prerenal: • Treat underlying cause • If volume depleted (see physical exam): NS boluses (500-1000ml fluid challenges) – can repeat until response (but need to monitor for fluid overload) • Avoid/be very cautious about giving lasix (again investigation of underlying cause should drive this decision). • Postrenal: • Treat underlying cause • Initiate Foley catheter (clear/flush catheter if already in place) • Obtain Renal Ultrasound to assess for upper urinary tract problems • Intrarenal: • Treat underlying causes (e.g. sever sepsis/shock)
SUMMARY • Verify urine output w/ definition of oliguria in mind. • If pt has a Foley catheter, flushing Foley is a good initial step. If no Foley, a PVR can help assess the need for Foley. • A focused chart review along with a focused history and physical can help clue in on the pathophysiology including pre-renal/intrinsic/post-renal causes. • Recognizing life threatening complications (e.g. hyperkalemia, acidosis, uremia) is an essential component of acute/early management. • Decreased urine output does NOT mean lasix deficiency. Administering lasix may actually exacerbate problem. However very specific causes may require lasix. • Fluid boluse(s) is a good initial step (be very cautious in CHF). • Ultimately, regardless of pathophysiology, treating underlying cause is key for both acute and long term management.