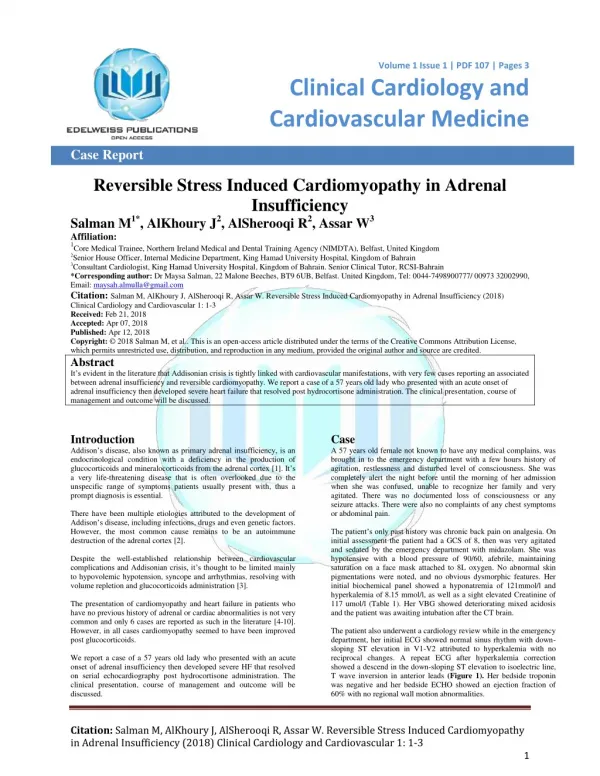
Acute Adrenal Insufficiency
Acute Adrenal Insufficiency. Dr. Sohail Inam FRCP (Ed), FRCP Consultant & Head, Division of Endocrinology Armed Forces Hospital Riyadh. CRH. AVP. Renin substrate. Kidney. Renin. ACTH. Angiotensin I. Angiotensin II. Cortisol. Aldosterone. Androgens. CRH. AVP. Renin substrate.

Acute Adrenal Insufficiency
E N D
Presentation Transcript
Acute Adrenal Insufficiency Dr. Sohail Inam FRCP (Ed), FRCP Consultant & Head, Division of Endocrinology Armed Forces Hospital Riyadh
CRH AVP Renin substrate Kidney Renin ACTH Angiotensin I Angiotensin II Cortisol Aldosterone Androgens
CRH AVP Renin substrate Kidney ACTH Renin Angiotensin I X Angiotensin II Cortisol Aldosterone Androgens
CRH AVP Renin substrate Kidney X Renin ACTH Angiotensin I Angiotensin II Cortisol Aldosterone Androgens
Acute Adrenal Insufficiency • Previous adrenal insufficiency • Previous normal adrenal function • Acute adrenal injury • Acute pituitary injury • Drug related effect • Functional adrenal insufficiency • Beware of previous corticosteroid use
Acute Adrenal InsufficiencyPresentation Non-specific • Hypotension • Postural • Recumbent • Abdominal pain • Electrolyte disturbances • Hypoglycemia
Acute Adrenal InsufficiencyPrecipitating factors • Omission of corticosteroids • Increased requirements • Infection • Physical stress • Drugs
Diagnosis • Measurement of adrenal hormones Cortisol • Primary versus central ACTH • Determine cause
DiagnosisCortisol • Random • 8-9 am level • Level during stress • Stimulated • ACTH • Hypoglycemia • CRH • Metyrapone
100 % chance of adrenal insufficiency 0 <83 650 9 am serum cortisol nmol/l
ACTH Stimulation Test • Standard (250 mcg) , Low dose (1mcg) • Can be performed any time though preferably 8-9 am. • 0, 30, 60 minute • Any value 550 nmol/l excludes adrenal insufficiency in non-critically ill patients • Test is abnormal in almost all patients with primary adrenal insufficiency & 90% individuals with central adrenal insufficiency
Pituitary Stimulation Tests • Insulin tolerance test (ITT) • Gold standard for central disease • Risk from hypoglycemia • CRH • Metyrapone • Other
Suspicion of AIApproach • ACTH stimulation test • ACTH measurement on basal sample
Acute AIManagement • Fluids • Glucocorticoids • Treat underlying cause
Fluid Therapy • Volume depends upon haemodynamic state & type of AI • Primary AI – hypovolemia (Salt wasting) • Central AI - euvolemia • 0.9% Saline • Beware of rapid change in Na • Dextrose to treat hypoglycemia
Steroid Therapy • Hydrocortisone drug of choice • Natural compound • Mineralocorticoid activity • Dose • No need to use large doses • 50 mg 6 hourly (avoid less frequent doses) • Taper dose early • No additional benefit of mineralocorticoids
“Low dose regime” 1350 Hydrocortisone 50 mg six hourly Arafah BM, JCEM 2006
Electrolyte Disturbance • Hyponatremia • 0.9% saline • Glucocorticoid Beware of rapid change in Na • Hyperkalemia • Fluids & hydrocortisone • Severe cases: NaHCO3, Glucose/insulin
Critical Illness Cortisol is a stress hormone and essential for survival • Metabolic effects Provision of energy • Haemodynamic effects • Salt & water retention • Increase presser response • Anti-inflammatory effects
CortisolCritical Illness Cortisol levels are elevated (2-3 times) • Increased secretion • Loss of diurnal variation • Decreased negative feedback • Decreased catabolism
CortisolCritical Illness Increased availability • Greater increase in Free Cortisol Decreased Binding (CBG, Albumin) • Increased tissue delivery Elastase • Increased tissue effect Up regulation of receptors
Neurogenic stimuli Adrenergic stimulation CRH Cytokines AVP ACTH Cortisol Aldosterone Androgens Tissue action
Cortisol in critical illnessDilemmas • How much is good? • Very high levels – deleterious? • Low levels – deleterious • Cortisol measurement? • Changes in free cortisol, hetrophil antibodies • Tissue modulation • No test to measure tissue effect
Issues with metanalysis • Small numbers • Measurement of cortisol • Major influence of one study • Almost 80% non-responders • Almost ⅓ had received etomidate • Not designed to test adverse effects • Duration & tapering of steroids
CORTICUS study • Non-responders had higher mortality • No difference in mortality between steroid and placebo group • Overall shock reversal rates higher in steroid group- not significant • Rates of super-infection were higher in the steroid group- NS • Hyperglycemia more common on steroids
AI in Critical IllnessApproach • Must not miss individuals with true cortisol deficiency • Definitive AI • Relative AI Treating such individuals could be life saving • Avoid unnecessary steroid therapy
Adrenal InsufficiencyCritical Illness • Routine testing not recommended • Actively screen those at high risk • ACTH stimulation test • Patients unresponsive to fluids & vasopressors merit trial of steroids
Cortisol in critical illnessHigh risk for adrenal insufficiency • Head injury • Known endocrine disease • Previous steroid use • Drugs (etomidate, ketoconazole, Medroxyprogesterone, megestrol) • HIV • Bleeding diathesis
Adrenal InsufficiencyCritical Illness Cut off values for cortisol • Basal • Cortisol <400 highly suggestive • Cortisol >810 (930) excludes AI • ACTH stimulation (normal values) • Increase of >250 nmol/l above baseline • Peak cortisol >930 nmol/l?