Download

1 / 35
440 likes | 1.02k Vues
ADRENAL GLAND: Congenital adrenal hyperplasia & adrenal insufficiency. Dr. Amnon Zung Pediatric Endocrinology Unit Kaplan Medical Center. Congenital Adrenal hyperplasia – the beginning. 21-hydroxylase deficiency Classic: female pseudohermaphroditism (DSD):

E N D
ADRENAL GLAND: Congenital adrenal hyperplasia & adrenal insufficiency Dr. Amnon Zung Pediatric Endocrinology Unit Kaplan Medical Center
Congenital Adrenal hyperplasia – the beginning • 21-hydroxylase deficiency Classic: female pseudohermaphroditism (DSD): At birth: urogenital sinus, labial fusion, clitoromegaly 75% are salt wasters Frequency:1:13,000 to 1:15,000 live births (based on 6.6 million newborn screened) Carrier state: 1:63 New York city: 1:100 / 1:7 Ashkenazi Jews: 1:27 Hispanics: 1:40 Slavs: 1:50 Italians: 1:300 • 11-ß hydroxylase deficiency Frequency: 1:100,000 (highest in Moroccan Jews)
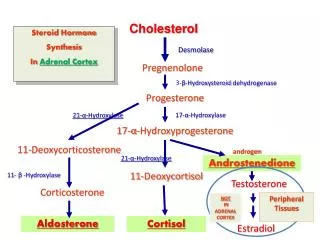
CAH – Molecular Genetics • 21-hydroxylase encoding gene: • Short arm of chromosome 6 • Two homologous genes: Cyp21B & Cyp21A (pseudogene) • 98% homology in exons (n=10); 96% in introns • About 50 mutations known today • Correlation & none-correlation of genotype\phenotype
CAH: genotype-phenotype correlation due to 21-hydroxylase deficiency • Patients are often compound heterozygotes • Phenotype is likely to reflect less severely allele • Mutation classification based on reduced activity: Severe Moderate Mild Severe SWSVNC Moderate SVSV NC Mild NC NC NC
CAH:Clinical features of different types S W S VNon-C Age at Dx M: 0-6m M:1.5-4y M: 0-18 y F: 0-1 m F: 0-2 y F: 0-18 y Genitalia: M: normal M: normal M: normal F: ambiguous F: ambig. F: clitoris Aldosterone normal normal Renin = or normal 17-OH P >600nmol/L 300-600 45-300 Testosterone Somatic growth -2 to –3 SD -1 to –2 SD nl to –1SD Enzymatic activity 0% 1% 20-50%
Classical CAH due to 21OH deficiency:clinical features • Postnatal period M & F: rapid somatic growth, bone age advancement early pubarche, early body odor, acne true precocious puberty M: increased penile size without testicular enlargment F:hirsutism, ovarian dyfunction (amenorrhea, dysmenorrhea)
Classical CAH: Salt wastingclinical features May lead to adrenal crisis by the 2nd week of life • Poor appetite, failure to thrive • Vomiting • Lethargy
Adrenal hyprplasia due to 21 hydroxylase deficiency: Diagnosis Diagnosis • Synacten (ACTH) stimualtion test: especially important to detect NC adrenal hyperplasia • Aldosterone, renin, Na, K: for CAH (SV/ SW)
Case report [2] • ACTH (Synacten) stimulation test 17-hydroxyprogesterone: > 75 nmol/L over the study Cortisol levels: up to 46 nmol/L • Skeletal age: 10 years & 3 months (with sesamoid bone !) • Plasma renin activity: 13.4
Adrenal hyprplasia due to 21 hydroxylas deficiency: Treatment • Children: hydrocortisone 10-20 mg/m2/d BID-TID • Adolescents & adults: prednisone 5-7.5 mg/d BID or dexamethasone 0.25-0.5 mg QD • Fludrocortisone (florinef) 0.1-0.2 md/day + Nacl 1-2gr/day (1gr = 17 meq Na) TREATMENT: PREDNISONE 1.25 BID + FLORINEF 0.1 mg + CLINIC VISIT A MONTH LATER
Adrenal hyprplasia due to 21 hydroxylase deficiency: treatment & follow-up Aims of treatment • Keeping 17OH-P at the upper normal limits (sometimes add MC for better suppression) • Avoid liquid hydrocortisone – better crush tablets • Avoid GC side effect: compromised growth, rapid weight gain, pigmented striae, osteopenia • Avoid MC side effects: hypertension, edema, tachycardia.
Adrenal hyprplasia due to 21 hydroxylase deficiency: treatment & follow-up Monitoring treatment • Check periodically 17OH-P, androstenedione (testosterone in girls & prepubertal boys) • PRA (for children treated with flurinef) Doses during stress • Wear warning bracelet • Triple GC dose on moderate to severe stress • When p.o. is not possible: IM/IV Solu-Cortef • At major surgery: IV hydrocortisone 100 mg/m2/day QID for 24 hr, than tapering over several days
Case report [3] 10 days before clinic visit, he stopped prednisone treatment 7 days before clinic visit, he developed high fever 1 day before clinic visit, he was brought to ER pulseless & with respiratory arrest. His BG was 4 mg%.
Adrenal insufficiency • Primary adrenal insufficiency (Addison disease) Low cortisol, low aldosterone, high ACTH • Secondary adrenal insufficiency Low cortisol, normal aldosterone, low ACTH
Adrenal insufficiency Glucocorticoids: • Modulate ACTH secretion ACTH elevation • Inotropy of heart muscle tachycardia, low stroke volume • Vascular response to beta agonists low vascular resistance • Antagonize insulin action hypoglycemia Mineralocorticoids: • Distal tubule sodium retention hyponatremia • Distal tubule potassium & hydrogen excretion hypokalemia & matabolic acidosis
Primary adrenal insufficiency • Autoimmune adrenal insufficiency 65% • Tuberculosis 20% • Other causes 15% • Fungi (histoplasmosis, blastomycosis, coccidio, crypto) • Adrenal hemorrhage (anti coagulants, DIC, trauma) • Metastases (breast, lung, stomach, colon, melanoma, lymphoma • Sarcoidosis • Amyloidosis • Adrenoleukodystrophy • AIDS • Congenital adrenal hyperplasia • Congenital unresponsiveness to ACTH • Medications (fluconazole, ketoconazole, phenytoin, rifampin)
Secondary adrenal insufficiency • Hypothalamic – pituitary – adrenal suppression • Glucocorticoids • Cushing syndrome • Lesions of the hypothalamus or pituitary gland • Neoplasm (pituitary tumor, metastases) • Craniopharyngioma • Infection (tuberculosis, actinomycosis, nocardia) • Head trauma
Glucocorticoid induced 2nd adrenal insufficiency • Depends on dose & duration • Should be anticipated in any patient who has been receiving > 30 mg of hydrocortisone per day for > 3 w Prednisolone (solomedrol) x 4 Prednisone (meticorten) x 5 Dexamethasone x 40 • Adrenal suppression can last up to 1 year !
Symptoms of adrenal insufficiency • Weakness & fatigue 100% • Anorexia 100% • Nausea, vomiting, diarrhea 50% • Muscle, joint & abdominal pain 10% • Postural dizziness 10% • Craving for salt • Headache • Memory impairment • depression
Signs of adrenal insufficiency • Weight loss 100% • Orthostatic hypotension 90% • Tachycardia • Fever • Hyperpigmentation 90% • Vitiligo 5%
Laboratory finding in adrenal insufficiency • Hyponatremia • Hyperkalemia • Metabolic acidosis (mild) • Hypoglycemia • Normochromic-normocytic anemia • Lymphocytosis • Eosinophilia • Elevated TSH levels
Adrenal insufficiency - treatment • In glucocorticoid-induced adrenal suppression: Maintenance dose x 3 to x 6: depends on severity of disease • In shock: 5% dextrose in normal saline • Hydrocortisone 50 – 100 mg qid • (Florinef 0.05 mg/ day)
CAH due to 11ß-HYDROXYLASE DEF • About 5-8% of CAH cases • Prevalence: 1:100,000 live births • In Jews from Morocco: 1;5000-1:7000 (R448H) • Two 11ß-hydroxylase isoenzymes: CYP11B1: 11ß hydroxylase 11 deoxycortisol to cortisol/ 11-DOC to corticosterone CYP11B2: aldosterone synthase 11-DOC to corticsterone 18-hydroxylase / 18 oxidase activity
CAH due to 11ß-HYDROXYLASE DEF Regulation of the 2 isoenzymes: • CYP11B1: ACTH • CYP11B2: Renin – Aldosterone System + K
11ß hydroxylase defucuency: Lab & Clinic • Mild to moderate hypertension (66%) • Hyperandrogenism • No correlation between hypertension & hyperandrogenism • High ACTH stimulated 11-DOC & 11-deoxycortisol (S) • Suppressed PRA + aldosterone • Hypokalemia/ muscle weakness (minority)
11ß hydroxylase defucuency: Treatment • Glucocorticoids • For long-standing hypertension: K-sparing diuretics: spironolactone Calcium-channel blockers: nifedipine (NO: Thiazides, ACE inhibitors)