Download
1 / 46
460 likes | 634 Vues
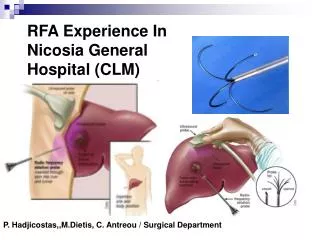
RFA Experience In Nicosia General Hospital (CLM). P. Hadjicostas,,M.Dietis, C. Antreou / Surgical Department. Liver Tumors (primary or metastatic) Resection: is the gold standard of treatment. BUT in only 9 – 27% in patients with HCC & 20% inpatients with Liver CRM’s.

E N D
RFA Experience In Nicosia General Hospital (CLM) P. Hadjicostas,,M.Dietis, C. Antreou / Surgical Department
Liver Tumors (primary or metastatic) • Resection: is the gold standard of treatment. • BUT in only • 9 – 27% in patients with HCC • & 20% inpatients with Liver CRM’s. • The 2nd cause of death • If untreated (6-18 months live) • 70% recurence after Resection • 50% recurence within the liver • The worsen development in a cancer patient
History:Thermal Cancer Therapy • Hot oil treatment of tumors described in 5000 y.o Egyptian papyrus • Tumor´´ cautery´´ used for numerous cancer types over past 400 years • Electrocautery destruction of superficial and endothelial malignancies over past 120 years • More recently, cryoablation, laser photocoagulation, radiofrequency ablation and microwave coagulation
Local Ablative therapy(unresectable Liver tumors) A. Percutaneous injection 1. Chemicals - Alcohol (P.E.I.T) - Acetic acid 2. Radio active isotopes 3. Hyperthermic agents - Saline - Water 4. Chemotherapeutic agents - Chemoembolization B. Percutaneous application of an energy source 1. Thermal ablation - Radiofrequency - Microwave (P.M.C.T) - Interstitial laser photocagulation 2. Cryoablation
“ A good local ablative method should be locally effective to the cancer, non-toxic to nontumorous liver, and easy and safe to administer”. “The endpoint of local ablation is complete tumor necrosis with a margin of tissue” Lau et al 2002
RFA is a new promising treatment for Liver tumors. “to heat and thereby kill tumor cells and normal surrounding parenchyma” Strasberg et al 2003 “thermal tissue destruction” Curley et al 2000 “…… What is not cured by knife is cured by fire” Heppocrates
The Cool-Tip™RF System Slide 7Ε
Useful Tips 2. Always place the end of the Cool Tip needle to the distant end of Lesion. Slide 5Δ
RF Ablation Technology Tissue response to Heat 100° C 90° C 80° C 70° C Cool Tip Minimum Target Temp 60° C Collagen denatures 50° C Thermal injury starts
RFA By Surgeon and in the OR • Friendly environment • Anesthesiologist is present • Continuous monitoring (BP, Pulse, ECG, Sat O2 ) • Arrhythmia • Hyperthermia/Sweating/ Discomfort • More analgesia • Maybe gen. anesthesia • Higher safety
RFA should be reserved for pts. • Unresected metastases/ Downsizing • Unable to tolerate lapatatomy for resection • BUT could challenged hepatectomy • New hepatic metastasis following liver resection( Elias 2002, Joosten 2007) • Limited central disease/hemihepatectomy( Evrard 2006,Abitabile 2007,Bremers 2007) • Small metastasis (Evrard 2007,Wagman 2007) • Solidary metastasis ( Oshowo 2003)
RFA • - percutaneously (65-75%) • Open Surgery • Laparoscopic • (Treatment approach individualized in any given patient)
Cost-effectiveness of RFA vs Hepatic Resection State Transition Decision Model – Disease Extent, Post Treatment Imaging Gazelle et al: radiology;2004:729
Morbitity of RFA Vs Resection Randomized Control Trials 7% 30%
Surgical Resection vs RFA (PCT) 180 Patients (HCC < 5cm) No Difference Annals of Surgery:Chen MS 243:March, 2006
Tension: Resection VS Ablation Open ResectionAblation Long Term Risk of Recurrence Short Term Risk of QOL impairment
N.G.H. RFA CLM Table • RFA performed 36 patients • Metastatic lesions 77 • Metastatic lesion / patient 1 – 5 • Metastatic lesion size 1 – 9cm
Patient pre-operative evaluation • Patient pre-operative evaluation from specialized team. (General surgeon, Oncologist, Pathologist, Radiologist) • Unresectional patients. Fits ablation criteria. • CT scan, occasional MRI. • Technical planning. (individualized) • Patient briefing, concept form.
Technical Method • Patient re-evaluation. • Operation theatre. • Presence of anesthesiologist, radiologist. • US guidance. • Single probe, triple probe, overlapping technique.
Follow up • Patient follow up evaluation from specialized team. • Ablation CT scan re-evaluation. (1-6 months)
N.G.H. RFA CLM Table • Minor Complications 2 / 36 (5.6%) • Local Recurrence 3 / 36 (8.3%) • Survival (months) 1 – 72m (32m)
N.G.H. RFA Survival Chart 92% / 12m 55% / 24m RFA 39% / 36m
93% / 12m 92% / 12m 59% / 24m 55% / 24m 42% / 36m 39% / 36m Abdalla et al, Annals of Surgery 2004
N.G.H. RFA Survival Chart p=0.01 52% / 36m Solitary tumor 20% / 36m >1 tumor
52% / 36m 68% / 36m 20% / 36m 43% / 36m Abdalla et al, Annals of Surgery 2004
N.G.H. RFA Survival Chart p=0.05 65% / 36m 16% / 36m ≤3cm >3cm
50% / 36m 65% / 36m ≤3cm 3 – 5cm <5cm Berber et al, Journal of Clinical Oncology 2005
Marginal Recurrence S/P-Hepatic Resection Not zero but 1.2- 10.4% ( Mulier 2008)
Conclusion • Minimally invasive method. Low complications. • Well tolerated. • Low cost effective. • Easily repeatable. • Local recurrence?